
Remember me








Currently, local anesthetic-induced systemic toxicity is treated with lipid emulsion, which is primarily used for parenteral nutrition.[1] Supportive treatments, which are used to alleviate central nervous and cardiovascular symptoms caused by toxicity due to other substances (including neuropsychiatric drugs without a specific antidote), include charcoal, gastric lavage, fluid administration, sodium bicarbonate, inotropic agents, vasopressors, anti-arrhythmic drugs, and defibrillation.[2,3] However, when supportive treatment does not improve the symptoms caused by neuropsychiatric drugs toxicity, lipid emulsion as adjuvant drug has been reported to be effective in ameliorating intractable central nervous system and cardiovascular system symptoms caused by toxic doses of antipsychotics and antidepressants.[2–4] In 2008, Siriari et al[5] reported a clinical case regarding lipid emulsion resuscitation of intractable cardiac arrest due to toxic doses of bupropion (an antidepressant) and lamotrigine (an anticonvulsant); this was the first successful lipid emulsion resuscitation for nonlocal anesthetic toxicity. Antidepressants, including amitriptyline and fluoxetine, and antipsychotics, such as quetiapine and haloperidol, produce corrected QT interval (QTc) prolongation, which leads to Torsade de Pointes, ventricular fibrillation, and cardiac arrest.[6] SMOFlipid was reported to reverse the decreased Glasgow Coma Scale (GCS) score and QTc prolongation induced by clozapine (an atypical antipsychotic) toxicity.[7] Intralipid increased the GCS scores of patients with acute toxicity caused by various nonlocal anesthetic drugs.[8] In addition, the time required to recovery from sevoflurane and isoflurane anesthesia was shortened by lipid emulsion in rats, and appeared to be mediated by lipid emulsion-mediated reduction of sevoflurane and isoflurane concentrations.[9] However, a systemic analysis of case reports regarding the effect of lipid emulsion on neuropsychiatric drug-induced toxicity, including antidepressants, antipsychotics, benzodiazepines (sedatives), and anticonvulsants, has not previously been reported. Moreover, a randomized controlled study regarding the effect of lipid emulsion on neuropsychiatric drug-induced toxicity in humans is impossible due to ethics concerns.[10] Thus, in this review, we analyzed case reports on lipid emulsion treatment for neuropsychiatric drug-induced toxicity retrieved from PubMed until December 20, 2023. The goal of this review was to investigate the effect of lipid emulsion on symptoms caused by neuropsychiatric drug toxicity, with a particular focus on QTc prolongation, decreased GCS scores, and the lipophilicity of drugs that more frequently require lipid emulsion treatment.
2. MethodsInstitutional review board approval was not needed because this was a narrative review using case reports.
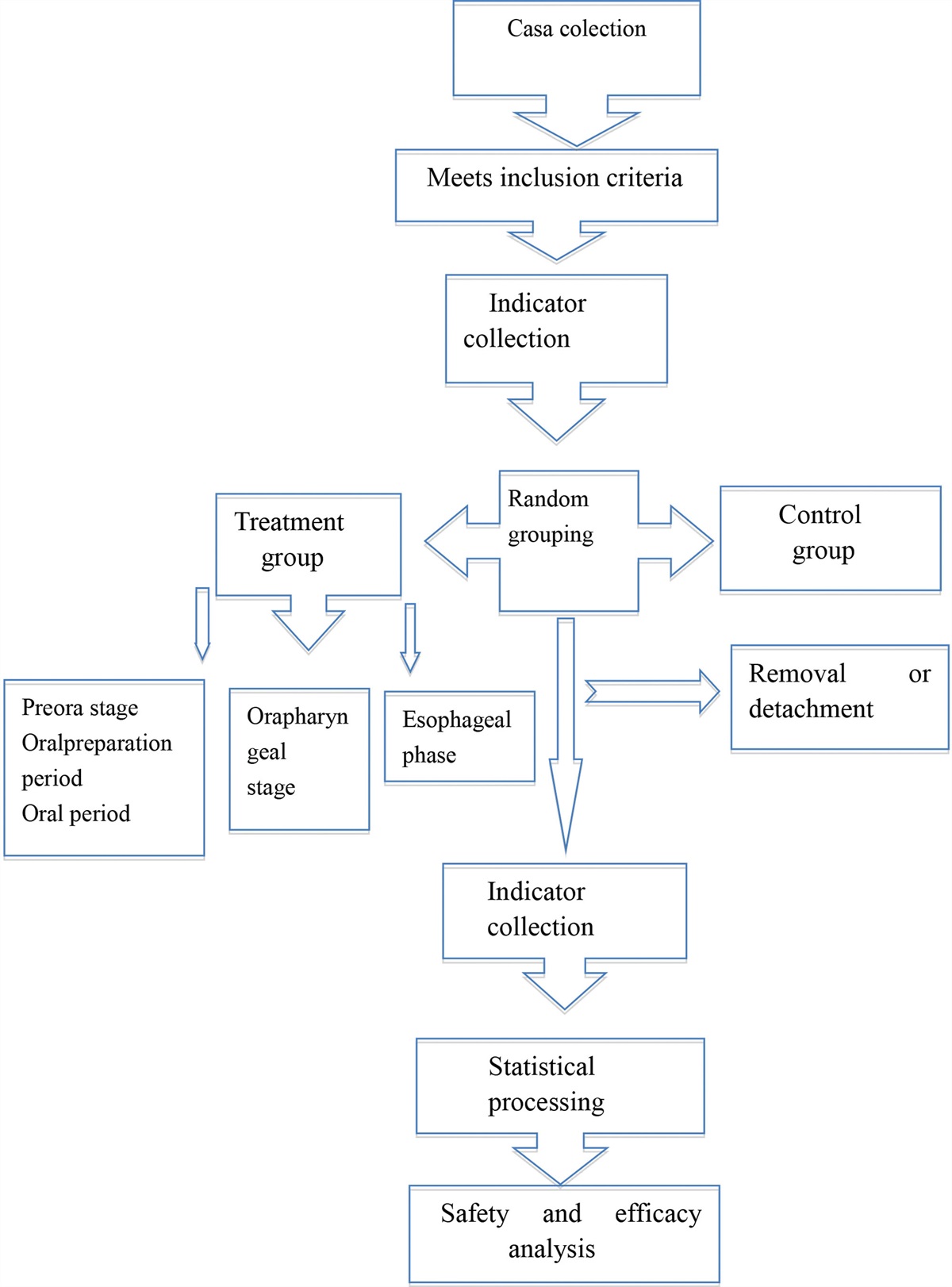
2.1. Case searchBased on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guideline,[11] the following terms were used to search for relevant case reports involving humans regarding the effect of lipid emulsion on drug toxicity caused by neuropsychiatric drugs until December 20, 2023: “antidepressant or antipsychotic drug or amitriptyline or bupropion or citalopram or desipramine or dosulepin or dothiepin or doxepin or escitalopram or fluoxetine or haloperidol or olanzapine or phenothiazine or quetiapine or risperidone or trazodone” and “lipid emulsion or Intralipid.” We retrieved a total of 1185 articles from PubMed (Fig. 1), which is Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram.
 Figure 1.:
Figure 1.: Flow chart for retrieving clinical case reports on lipid emulsion treatment as an adjuvant therapy for systemic neuropsychiatric (antidepressants, antipsychotics, benzodiazepines, and anticonvulsants) drug toxicity based on a PubMed keyword search. “n” indicates the number of articles.
2.2. Eligibility criteriaAfter removing duplicate articles (n = 374), 811 articles remained. A further 761 articles were excluded for the following reasons: no case report regarding lipid emulsion therapy, review article, systemic review, nonhuman cases, letter to the editor (not case report), and/or an original clinical and laboratory research article (Fig. 1). Finally, 50 articles were included in the analysis. As 1 article contained 2 patients and another article contained 10 patients, the 50 articles included 60 patients (Fig. 1).
2.3. Data extractionPre- and post-lipid emulsion treatment QTc intervals and GCS scores were obtained from each case report based on measurements just before and after the administration of lipid emulsion, respectively. QTc intervals were calculated using the Bazett formula (QTc = QT/RR1/2).[6] All other data, including age, sex, underlying diseases, neuropsychiatric drugs, dosage, lipid emulsion treatment information, improvement of symptoms, and outcomes, were obtained from the case reports. Log P (octanol/water partition coefficient) was obtained from PubChem.[12]
2.4. Statistical analysisNormality tests for all data, which included log P of the drug, GCS score, and QTc, were performed using Shapiro–Wilk tests (Prism 5.0; GraphPad Software, San Diego, CA). The effect of lipid emulsion on GCS score was analyzed using Wilcoxon signed-rank tests. The effect of lipid emulsion on QTc prolongation was analyzed using paired Student’s t tests. The log P values of the groups which required more than or less than 3 lipid emulsion treatments were compared using the Mann–Whitney test. P values below .05 indicate statistical significance.
3. Results 3.1. Sex, age, underlying disease, and drugsThe numbers of male and female patients (total patients: 60) with systemic neuropsychiatric drug-induced toxicity who underwent lipid emulsion treatment as an adjuvant drug were 20 (33.33%) and 37 (61.66%), respectively (Table 1). The age distribution was as follows (Table 1): 20–29 years (16 patients, 26.6%), 10–19 years (10 patients, 16.6%), 30–39 years (10 patients, 16.6%), 50–59 years (9 patients, 15%), 40–49 years (8 patients, 13.3%), 60–69 years (3 patients, 5%), and <10 years (2 patients, 3.3%). The incidence of underlying diseases were as follows (Table 1): depression (18 patients, 30%), bipolar disorder (5 patients, 8.33%), schizophrenia (3 patients, 5%), and epilepsy (2 patients, 3.33%). Two patients did not have any underlying diseases. The drugs that caused toxicity, which were mainly neuropsychiatric drugs, were as follows (n = 39; Table 1): antidepressants including amitriptyline, nortriptyline, dosulepine (dothiepine), doxepine, citalopram, escitalopram, sertraline, fluoxetine, venlafaxine, bupropion, mirtazapine, and trazodone; antipsychotics including olanzapine, quetiapine, chlorpromazine, haloperidol, aripiprazole, amisulpride, zopiclone, and paliperidone; benzodiazepines including diazepam, clonazepam, bromazepam, and alprazolam; anticonvulsants including pregabalin, gabapentin, and lamotrigine; and other drugs including metoprolol, propranolol, cyclobenzapine, hydroxyzine, nifedipine, quinapril, aspirin, valsartan, ibuprofen, insulin, amoxicillin, and clonidine. The specific drugs which most frequently caused neuropsychiatric drug toxicity (total number of drugs including duplicates: 109) and required lipid emulsion treatment as an adjuvant drug were as follows (Table 1): amitriptyline (19.2%) > quetiapine (11%) > venlafaxine (6.4%) > citalopram or olanzapine (5.5%) > lamotrigine or bupropion (4.6%) > trazodone (3.7%) > dosulepin or sertraline or fluoxetine (2.8%) > zopiclone or escitalopram or cyclobenzaprine or diazepam or metoprolol or gabapentin (1.8%) > others (0.9%).
Table 1 - Lipid emulsion treatment for toxicity caused by neuropsychiatric drugs (e.g., antidepressants, antipsychotics, benzodiazepines, and anticonvulsants). Case no. Sex Age Underlying disease Drug Dosage Log P Pre-LE QTc Pre-LE GCS Kind of LE Post-LE QTc Post-LE GCS Improved symptoms Outcome 1[13] F 28 Depression Amitriptyline 3.7 g 4.92 475 ms N/A (coma) 20% LE 441 ms WNL CNS, CV R 2[14] F 77 Depression Trazodone 4.5 g 2.68 540 ms 3 20% Intralipid 411 ms 10 CNS, CV R 3[15] F 15 N Bupropion 1650–9000 mg 3.6 461 ms 11 20% Intralipid N/A N/A CNS, CV R 4[16] N/A 25 Depression Amitriptyline
Comments (0)