
Remember me





Irrespective of mechanism, alcohol-related injury has a high prevalence within the trauma patient population. Excessive alcohol use and dependence puts hospitalized patients at risk for alcohol withdrawal syndrome (AWS) following admission and relative abstinence. The clinical diagnosis involves a myriad of symptoms including tachycardia, anxiety, diaphoresis, altered mental status, and tremors with progression to seizures in delirium tremens. Even patients with minor injuries and with negative admission blood alcohol concentration have a significant incidence of AWS. For trauma patients, developing AWS has been shown to increase morbidity and cost through increased ventilator days, pneumonia complications, unplanned intensive care unit (ICU) admissions, ICU days, and hospital days.1–5
Alcohol affects the central nervous syndrome through multiple neuromodulators and cellular receptors. Specifically, it increases the inhibitory effects of γ-aminobutyric acid (GABA) while simultaneously inhibiting N-methyl-d-aspartate receptors. This results in an upregulation of these receptors and subsequent increased stimulation of glutamate when alcohol is no longer present, resulting in a hyperexcitable neurologic state.6 Alcohol withdrawal syndrome is managed with supportive care and pharmacological measures, which have historically included benzodiazepines. Benzodiazepines have proven efficacious but are associated with a significant adverse effect profile. Specific to hospitalized patients, a 2016 study associated initiation of benzodiazepines and dose escalation with an increased risk of inpatient falls.7 Benzodiazepine-sparing protocols for both AWS prophylaxis and treatment exist within the medical literature, but the data to support their use in the trauma population are limited and primarily use phenobarbital.8–10
Our group reviewed the AWS risk screening questionnaire published by Maldonado et al.11,12 in 2014 and their group's subsequent benzodiazepine-sparing protocol and modified the pharmacologic algorithm for use on our trauma service. Our aim was to create a protocol for management of AWS within the trauma population that incorporated risk stratification, prophylaxis, and treatment while also considering the physiologic effects of injury. We hypothesized that this protocol would identify patients at risk for AWS and safely manage their symptoms while decreasing the need for benzodiazepine dosing.
PATIENTS AND METHODSA retrospective cohort study of adult (18 years or older) trauma patients who either screened positive for alcohol dependence risk based on clinical assessment or were treated for AWS from January 2018 to August 2020 was conducted at a single, tertiary academic Level 1 trauma center. Historically, patients were identified to be at risk if they presented with a positive blood alcohol, a positive Alcohol Use Disorders Identification Test—Concise score or had a positive standardized bedside nurse screen. Patients at risk were treated conventionally with benzodiazepines for AWS based on clinical diagnosis with a symptoms-triggered pathway. Patients with a Clinical Institute Withdrawal Assessment for Alcohol, revised (CIWA-Ar), score of >8 received 2 mg of lorazepam (orally or intravenously) every 4 hours as needed. Patients with CIWA-Ar score of ≥15 were treated with 2 mg of lorazepam every hour as needed. Occasionally, patients deemed at very high risk were given chlordiazepoxide for treatment or prevention of AWS. In 2019, we implemented a benzodiazepine-sparing (BS) pathway that primarily used gabapentin and clonidine. All trauma patients were screened at admission for AWS risk using the traditional metrics as well as with the Prediction of Alcohol Withdrawal Severity Scale (Fig. 1). Based on the results of initial screen, patients were assigned to (1) no monitoring for AWS, (2) monitoring by CIWA-Ar or the modified Minnesota Detoxification Scale (mMINDS) alone, (3) a prophylactic pharmacologic arm, or (4) a treatment pharmacologic arm based on a benzodiazepine-sparing protocol (Fig. 2). Thus, our study sample was divided into two groups based upon preprotocol AWS treatment with benzodiazepines (conventional [CONV]) and postprotocol AWS management with the BS protocol. All patients during the study period identified to be at risk for AWS by the methods described previously were included. Patients younger than 18 years and those with no risk factors for AWS were excluded. Additional data were obtained from the electronic medical record for all patients including demographics, admission date, discharge date, CIWA-Ar scores during admission, mMINDS scores during admission, ICU length of stay (LOS), ventilator days, morphine milligram equivalent doses, and lorazepam equivalent doses. Significant withdrawal was defined as CIWA-Ar or mMINDS score of ≥15 at any time during admission. Outcomes examined include morphine milligram equivalent dosing rates, lorazepam equivalent dosing rates, CIWA-Ar/mMINDS scores, hospital and ICU LOS, and ventilator days. Categorical data were compared with Pearson's χ2 or Fisher's exact test, and continuous data, with Wilcoxon-Mann-Whitney test and Student's t test. A p value of <0.05 was considered significant. Analyses were performed with IBM SPSS Statistics for Windows, version 27.0 (IBM Corp., Armonk, NY). The study was approved with a waiver of consent from the institutional review board (IRB00067590). The STrengthening the Reporting of OBservational studies in Epidemiology guideline was used to ensure proper reporting of methods, results, and discussions (Supplemental Digital Content, Supplementary Data 1, https://links.lww.com/TA/D371).
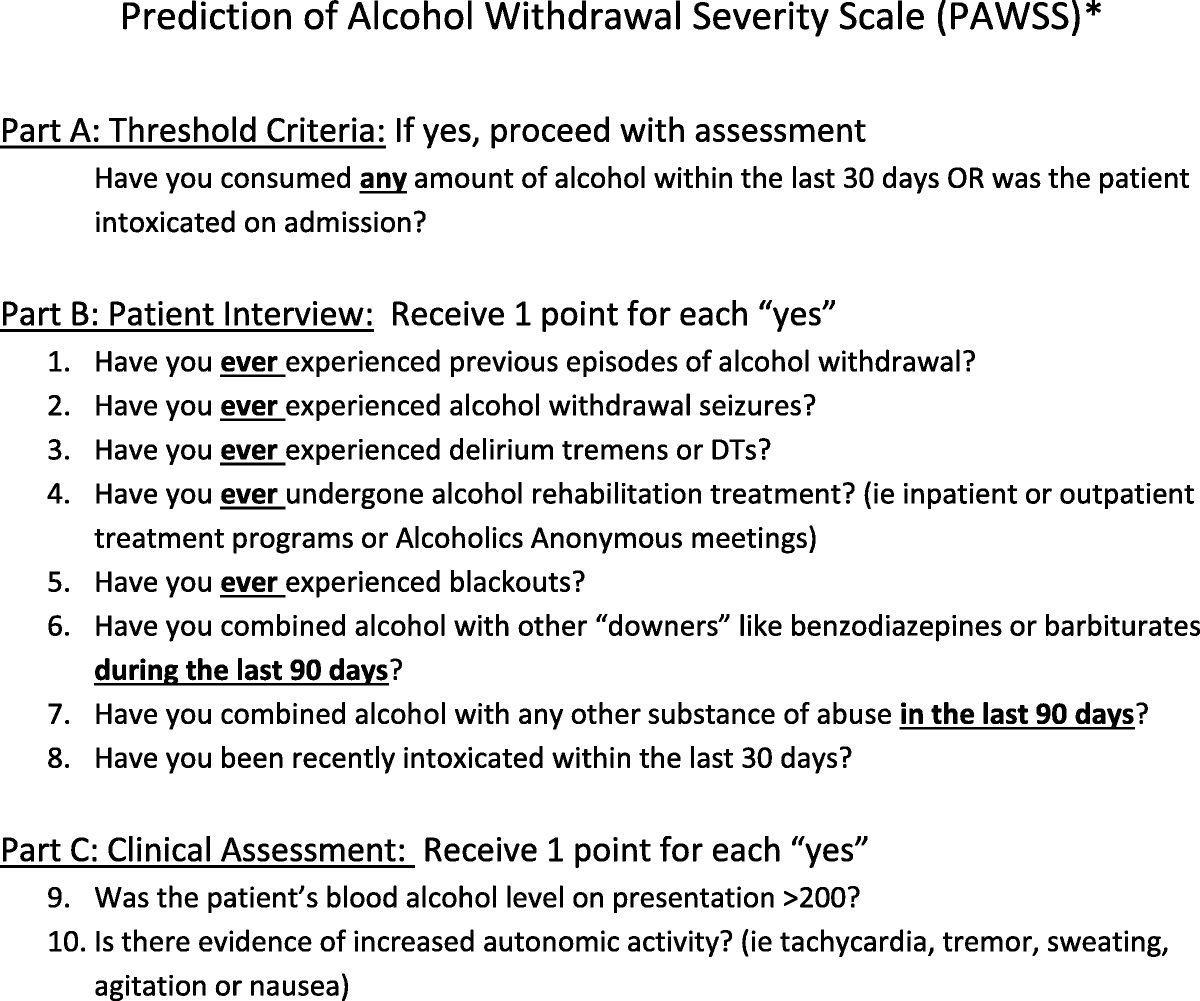
 Figure 1:
Figure 1: Predictive Alcohol Withdrawal Severity Scale. *Maldonado JR, Sher Y, Ashouri JF. The “Prediction of Alcohol Withdrawal Severity Scale” (PAWSS): systematic literature review and pilot study of a new scale for the prediction of complicated alcohol withdrawal syndrome. Alcohol 2014;45(4):375–9.
 Figure 2:
Figure 2: Benzodiazepine-sparing alcohol withdrawal protocol.
RESULTSOf 10,440 trauma patients during the study period, 522 were identified to be at risk for AWS (387 CONV and 134 BS). The two groups were similar in regards to male sex (CONV, 83.7% vs. BS, 85.1%; p = 0.71), age (CONV, 53 years vs. BS, 50 years; p = 0.51), blunt mechanism (CONV, 90.2% vs. BS, 93.3%; p = 0.37), Injury Severity Score (CONV, 13 vs. BS, 16; p = 0.10), and EtOH on arrival (CONV, 99 vs. BS, 149 mg/dL; p = 0.06). Table 1.
Conventional (n = 387) BS (n = 134) p Male sex, n (%) 324 (83.7) 114 (85.1) 0.712 Blunt mechanism, n (%) 349 (90.2) 125 (93.3) 0.367 Age, median (IQR) 53 (39–61) 50 (40–60) 0.51 Admission HR, median (IQR) 92 (81–105) 96 (79–111) 0.35 Admission SBP, median (IQR) 130 (116–148) 132 (112–149) 0.67 Admission GCS, median (IQR) 15 (14–15) 15 (13.75–15) 0.08 ISS, median (IQR) 13 (9–20) 16 (9–22) 0.10 Admission EtOH, mg/dL, median (IQR) 99 (0–210) 149 (0–227) 0.06HR, heart rate; GCS, Glasgow Coma Scale; IQR, interquartile range; ISS, Injury Severity Score; SBP, systolic blood pressure.
The overall rate of significant withdrawal, defined as CIWA-Ar or mMINDS score of ≥15, was similar between groups (CONV, 24.5% vs. BS, 26.9%; p = 0.59). However, BS patients had a lower daily CIWA-Ar max compared with CONV patients (CONV, 1.5 vs. BS, 2.7; p = 0.04). Morphine milligram equivalent per day was similar between patients in the CONV and BS groups (CONV, 31.5 mg vs. BS, 33.4 mg; p = 0.52). However, mean lorazepam equivalents per day was significantly lower for patients on the BS pathway (CONV, 1.14 vs. BS, 0.23 mg; p < 0.01). Length of stay and ventilator days were similar between groups. Table 2. In a subgroup of patients who experienced significant withdrawal, the difference in mean lorazepam equivalents per day was even more robust (CONV, 2.4 vs. BS, 0.4 mg/d; p < 0.01). Table 3.
TABLE 2 - Outcomes of Patients at Risk for AWS Conventional (n = 387) BS (n = 134) Withdrawal at any time point, n (%) 95 (24.5) 36 (26.9) 0.594 Mortality, n (%) 8 (2.1) 4 (3.0) 0.519 Hospital LOS, median (IQR), d 6 (3–13) 7 (3–12) 0.33 ICU LOS, median (IQR), d 1 (0–3) 2 (1–5) <0.01 CIWA-Ar max 5 (1–14) 4 (1–11) 0.12 CIWA-Ar daily max 2.7 (0.4–6.2) 1.5 (0.3–4.5) 0.04 mMINDS max 6.5 (2–19) mMINDS daily max 4 (2–11.6) CIWA-Ar/mMINDS max 5 (1–14) 5 (2–16) Mean morphine equivalents, mean (SD), mg 250.5 (385.6) 277.3 (402.1) 0.49 Mean morphine equivalents adjusted for LOS, mean (SD), mg/d 31.5 (31.0) 33.6 (28.3) 0.49 Mean lorazepam equivalents, mean (SD), mg 10.0 (23.3) 1.7 (5.3) <0.01 Mean lorazepam equivalents adjusted for LOS, mean (SD), mg 1.1 (2.5) 0.2 (0.6) <0.01There were no reported adverse events in the BS group. In rare instances, clonidine dose was reduced or discontinued in the BS because of relative hypotension, but this did not result in any complications (acute kidney injury, new vasopressor, etc.).
DISCUSSIONIn our study, we demonstrate the implementation of a benzodiazepine-sparing pathway to prevent and treat AWS. In the trauma population, a high percentage of hospitalized patients have some measure of alcohol use disorder that varies in severity and chronicity. Although multiple pharmacologic strategies for management have been proposed and studied, no optimal strategy for management, prevention, and risk stratification has been clearly defined in the literature. Our protocol uses gabapentin, clonidine, and valproic acid as primary agents for prophylaxis and treatment of AWS and avoids benzodiazepines, known for their adverse effect profile. In addition to sedation effects, administration of benzodiazepines has been associated with developing delirium in surgical ICU and trauma ICU patients, as well as postoperative patients.13,14
Our protocol relies heavily on gabapentin, which acts as a GABA modulator and has been shown by Mason et al.15 in a 2014 randomized controlled trial to effectively treat alcohol dependence in the primary care setting with a safe adverse effect profile. Gabapentin administration indirectly modulates GABA neurotransmission and has been found to mediate central nervous system disequilibrium that occurs in AWS.15 In a double-blind randomized clinical trial published by Anton et al.16 in 2020, gabapentin was shown to be superior to placebo in managing heavy alcohol use and those with prior AWS symptoms. Furthermore, gabapentin was also shown to be superior to lorazepam in a 2009 randomized control trial examining outpatient management of alcohol withdrawal.17 In addition, clonidine and dexmedetomidine, a drug with a similar structure to clonidine but higher selectivity for the α-2 receptor, have efficacy as combination treatments to treat AWS.18–20 Given the findings that AWS severity correlates with the amount of released norepinephrine, agents that reduce norepinephrine have a role in its prevention and treatment. Both of these agents are α-adrenergic agonists and inhibit presynaptic release of glutamate, aspartate, and norepinephrine. Multiple randomized controlled trials have demonstrated clonidine's efficacy in treating AWS. Dexmedetomidine has been found to be a useful adjunct for treatment of AWS but should be avoided as a single-agent approach.5 Our study supports the findings of these previously published studies. As outlined in our protocol, the provider may choose between gabapentin and clonidine for prophylaxis when initiating the pathway. Our group strongly prefers gabapentin because it is synergistic with our multimodal approach to pain control.
The BS pathway is unique in that it is a continuum for both prevention and treatment of AWS. Most published pathways are aimed at the treatment of AWS, but the pathway described here within is both preventative and therapeutic. Early recognition of the risk for alcohol withdrawal and empiric prophylaxis for prevention was recently recommended and emphasized in an American Association for the Surgery of Trauma Critical Care Clinical Consensus document.5 In addition, BS has the major advantage of being fixed, scheduled dosing of medications. This contrasts with most protocols that rely on symptom-triggered or pro re nata dosing. This allows for much less subjectivity in dosing regimens, and all medications can be administered in either ICU or ward settings. Patients can be escalated on the pathway for an elevated CIWA-Ar or mMINDS, but it is a fixed dose adjustment or addition of a medication, not a pro re nata dose. There has been significant recent interest in using phenobarbital for treating AWS, but our protocol differs in that it does not use barbiturates.8–10,21,22 While phenobarbital appears to be safe and effective, it requires intense monitoring, most often in an ICU setting. In addition, it is primarily administered for active withdrawal, although there are some data that suggest that it is feasible in the prevention of AWS.8,10 Although phenobarbital has a role in treating severe AWS, the advantage of the BS pathway over use of phenobarbital is that our pathway potentially prevents AWS through the initiation of medications for high-risk patients before signs and symptoms of AWS and the pathway requires less intense monitoring. Furthermore, as mentioned previously, many institutions require phenobarbital to be administered in an ICU setting, which is not a requirement with our protocol. Our protocol is also novel in that it has a clear pathway for escalation, a benefit that is missing from many existing protocols. Phenobarbital is clearly efficacious in the treatment of severe AWS, but we believe that our pathway offers a simplistic, benzodiazepine-sparing approach that accommodates the vast majority of patients. Proponents of both our protocol and a phenobarbital-based protocol generally agree that the avoidance of benzodiazepines is a major advancement in the care of AWS. In the future, we hope to compare our pathway with a phenobarbital-based pathway.
Historically, close monitoring of CIWA-Ar scores, particularly in the first 24 to 48 hours after admission, has played an important role in identifying AWS. However, CIWA-Ar assessment can be problematic and prohibitively subjective in the critically ill. Fortunately, mMINDS, validated for use in critically ill patients, correlates strongly with CIWA-Ar.23 This makes it possible to comfortably use both scoring tools within our current benzodiazepine-sparing protocol. Currently, our institution uses mMINDS in the ICU setting and CIWA-Ar on the wards. Based on the available literature, we allow these to be interchanged.
The present study contributes to several decades of research into the optimal management of AWS in hospitalized patients while focusing on the trauma population. While our study does not conclusively demonstrate superiority of a benzodiazepine-sparing pathway, we have demonstrated several key findings. First, this study supports the feasibility of the implementation of a pathway that addresses both the prevention and treatment of AWS and avoids the use of benzodiazepines and does not use phenobarbital. In addition, patients in the BS group had lower daily CIWA-Ar scores. Although we did not examine the impact lower scores had on the patients or the medical team, a reduction in CIWA-Ar scores means that the patient experienced fewer negative symptoms related to withdrawal. Fewer symptoms are likely to increase patient satisfaction and recovery while simplifying the overall management of the patient for the medical team.
In this study, we did not demonstrate a decrease in hospital or ICU LOS, potentially explained by a policy to admit all patients at substantial risk for AWS to the ICU. Since the conclusion of the study, as a result of the safety of the medications used and increased provider awareness and education, we have changed this policy and now allow these patients to be admitted to the ward, which may affect ICU LOS in future studies. Despite no decrease in LOS, using fewer benzodiazepines could affect patients in other positive ways. In a systemic review of benzodiazepine use and neuropsychiatric outcomes in the ICU, Kok et al.24 reported that most studies indicate that benzodiazepine use in the ICU is associated with symptoms related to posttraumatic stress disorder, anxiety, depression, and cognitive dysfunction, sometimes months after discharge. While these symptoms may not negatively impact LOS, it is likely they will impact quality of life for patients.
Our study has several limitations, including single-center, retrospective review, nonrandomized sample, and relatively small sample size. Our study is not sufficiently powered to detect a difference in AWS or severity between groups. In addition, with the implementation of our BS pathway, we introduced new screening tools (Prediction of Alcohol Withdrawal Severity Scale) and monitoring mechanisms (mMINDS), which may influence the data.
Implementing a benzodiazepine-sparing prophylaxis and treatment protocol that primarily uses clonidine and gabapentin for trauma patients at risk of AWS appears to be feasible, safe, and vastly reduces the need for benzodiazepines in this population. Future studies will evaluate the impact of avoiding benzodiazepines for the prevention and management of AWS in the trauma population and will compare our protocol with one that is phenobarbital based.
AUTHORSHIPM.A.M., T.M., K.A.R., M.C., E.H.S., and A.M.N. contributed in the literature search. M.A.M., A.M.N., P.R.M., G.R.S., R.S.M., J.J.H., and K.A.R. contributed in the study design. M.A.M., A.M.N., K.A.R., T.M., and M.C. contributed in the data collection. M.A.M. and A.M.N. contributed in the data analysis. M.A.M., A.M.N., G.R.S., and P.R.M. contributed in the data interpretation. M.A.M., A.M.N., and E.H.S. contributed in the writing. M.A.M., P.R.M., K.A.R., G.R.S., R.S.M., E.H.S., J.J.H., and A.M.N. contributed in the critical revision.
DISCLOSUREConflicts of Interest: Author Disclosure forms have been supplied and are provided as Supplemental Digital Content (https://links.lww.com/TA/D372).
REFERENCES 1. Ng C, Fleury M, Hakmi H, Bronson B, Vosswinkel JA, Huang EC, et al. The impact of alcohol use and withdrawal on trauma outcomes: a case control study. Am J Surg. 2021;222(2):438–445. 2. Bard MR, Goettler CE, Toschlog EA, Sagraves SG, Schenarts PJ, Newell MA, et al. Alcohol withdrawal syndrome: turning minor injuries into a major problem. J Trauma. 2006;61(6):1441–1445 discussion 1445-6. 3. Jawa RS, Stothert JC, Shostrom VK, Yetter DL, Templin HR, Cemaj SK, et al. Alcohol withdrawal syndrome in admitted trauma patients. Am J Surg. 2014;208(5):781–787. 4. Ahmed N, Kuo Y. Alcohol withdrawal syndrome in trauma victims. Under appreciated costly event. Am J Surg. 2021;222(3):506–507. 5. Seshadri A, Appelbaum R, Carmichael SP 2nd, Farrell MS, Filiberto DM, Jawa R, Kodadek L, Mandell S, Miles MVP, Paul J, Robinson B, Michetti CP. Prevention of alcohol withdrawal syndrome in the surgical ICU: an American Association for the Surgery of Trauma Critical Care Committee Clinical Consensus Document. Trauma Surg Acute Care Open. 2022;7(1):e001010. 6. Turner RC, Lichstein PR, Peden JG Jr., Busher JT, Waivers LE. Alcohol withdrawal syndromes: a review of pathophysiology, clinical presentation, and treatment. J Gen Intern Med. 1989;4(5):432–444. 7. Skinner BW, Johnston EV, Saum LM. Benzodiazepine Initiation and Dose Escalation. Ann Pharmacother. 2017;51(4):281–285. 8. Nejad S, Nisavic M, Larentzakis A, Dijkink S, Chang Y, Levine AR, de Moya M, Velmahos G. Phenobarbital for acute alcohol withdrawal management in surgical trauma patients—a retrospective comparison study. Psychosomatics. 2020;61(4):327–335. 9. Kip LM, Forni A, Dorfman JD, Li I. Evaluation of phenobarbital for prevention of alcohol withdrawal in trauma patients. J Trauma Acute Care Surg. 2023;95(4):573–576. 10. Ammar MA, Ammar AA, Rosen J, Kassab HS, Becher RD. Phenobarbital monotherapy for the management of alcohol withdrawal syndrome in surgical-trauma patients. Ann Pharmacother. 2021;55(3):294–302. 11. Maldonado JR, Sher Y, Das S, Hills-Evans K, Frenklach A, Lolak S, et al. Prospective validation study of the Prediction of Alcohol Withdrawal Severity Scale (PAWSS) in medically ill inpatients: a new scale for the prediction of complicated alcohol withdrawal syndrome. Alcohol Alcohol. 2015;50(5):509–518. 12. Maldonado JR. Novel algorithms for the prophylaxis and management of alcohol withdrawal syndromes—beyond benzodiazepines. Crit Care Clin. 2017;33(3):559–599. 13. Pandharipande P, Cotton BA, Shintani A, Thompson J, Pun BT, Morris JA Jr., et al. Prevalence and risk factors for development of delirium in surgical and trauma intensive care unit patients. J Trauma. 2008;65(1):34–41. 14. Marcantonio ER, Juarez G, Goldman L, Mangione CM, Ludwig LE, Lind L, et al. The relationship of postoperative delirium with psychoactive medications. JAMA. 1994;272(19):1518–1522. 15. Mason BJ, Quello S, Goodell V, Shadan F, Kyle M, Begovic A. Gabapentin treatment for alcohol dependence: a randomized clinical trial. JAMA Intern Med. 2014;174(1):70–77. 16. Anton RF, Latham P, Voronin K, Book S, Hoffman M, Prisciandaro J, et al. Efficacy of gabapentin for the treatment of alcohol use disorder in patients with alcohol withdrawal symptoms: a randomized clinical trial. JAMA Intern Med. 2020;180(5):728–736. 17. Myrick H, Malcolm R, Randall PK, Boyle E, Anton RF, Becker HC, et al. A double-blind trial of gabapentin versus lorazepam in the treatment of alcohol withdrawal. Alcohol Clin Exp Res. 2009;33(9):1582–1588. 18. Spies CD, Otter HE, Hüske B, Sinha P, Neumann T, Rettig J, et al. Alcohol withdrawal severity is decreased by symptom-orientated adjusted bolus therapy in the ICU. Intensive Care Med. 2003;29(12):2230–2238. 19. Awissi DK, Lebrun G, Coursin DB, Riker RR, Skrobik Y. Alcohol withdrawal and delirium tremens in the critically ill: a systematic review and commentary. Intensive Care Med. 2013;39(1):16–30. 20. Linn DD, Loeser KC. Dexmedetomidine for alcohol withdrawal syndrome. Ann Pharmacother. 2015;49(12):1336–1342. 21. Smith JT, Sage M, Szeto H, Myers LC, Lu Y, Martinez A, et al. Outcomes after implementation of a benzodiazepine-sparing alcohol withdrawal order set in an integrated health care system. JAMA Netw Open. 2022;5(2):e220158. 22. Nisavic M, Nejad SH, Isenberg BM, Bajwa EK, Currier P, Wallace PM, et al. Use of phenobarbital in alcohol withdrawal management - a retrospective comparison study of phenobarbital and benzodiazepines for acute alcohol withdrawal management in general medical patients. Psychosomatics. 2019;60(5):458–467. 23. Littlefield AJ, Heavner MS, Eng CC, Cooper DA, Heavner JJ, Kurtz JM, et al. Correlation between mMINDS and CIWA-Ar scoring tools in patients with alcohol withdrawal syndrome. Am J Crit Care. 2018;27(4):280–286. 24. Kok L, Slooter A, Hillegers M, van Dijk D, Veldhuijzen D. Benzodiazepine use and neuropsychiatric outcomes in the ICU: a systematic review. Crit Care Med. 2018;46(10):1673–1680.
Comments (0)