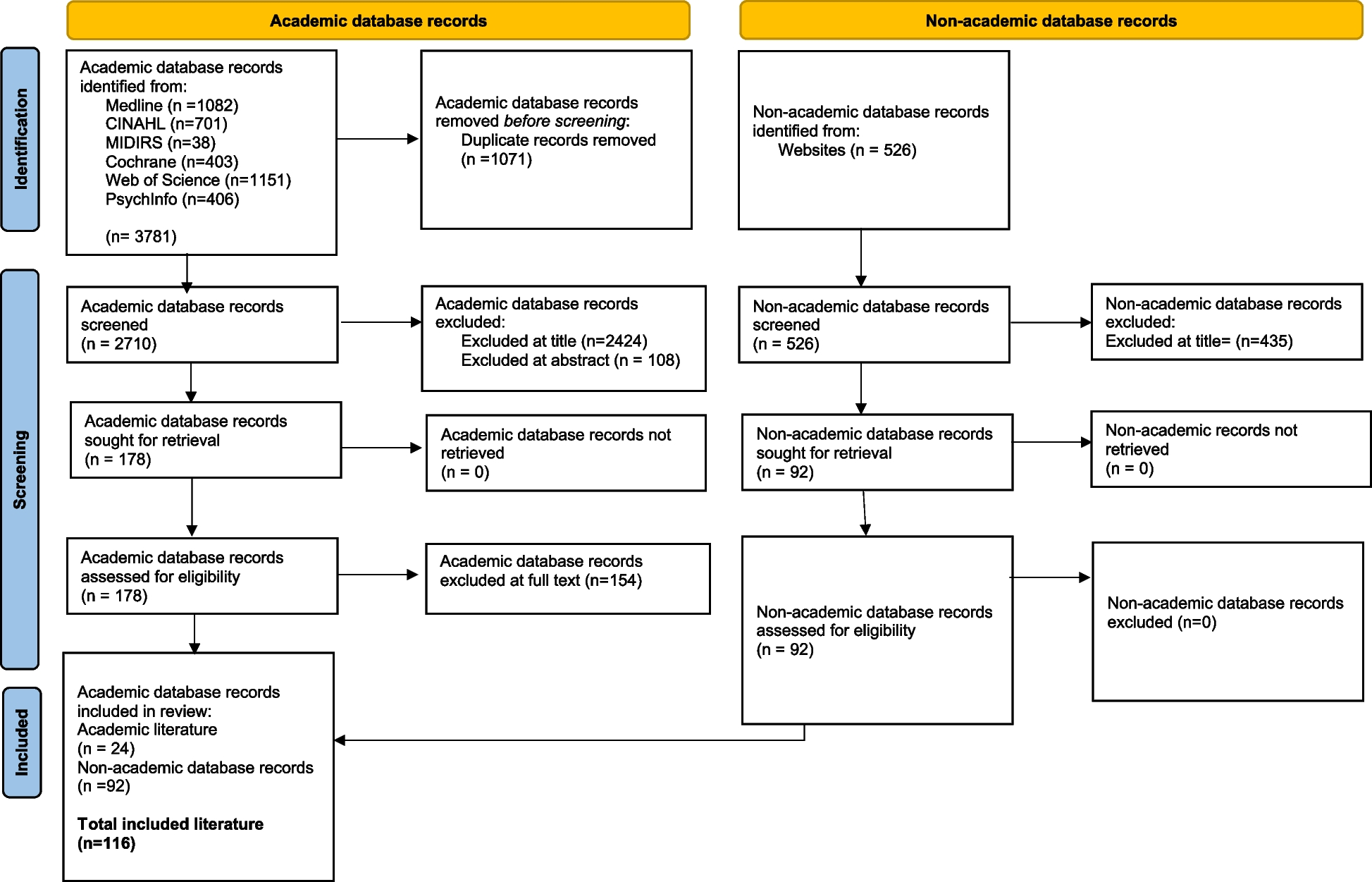
Database searches produced a total of 1037 publications. After duplicates were removed, 539 papers were screened by title and abstract; 466 papers were removed as their content did not meet the inclusion criteria. The full text of the remaining 73 papers were assessed for eligibility with 57 excluded at this stage (see Supplementary Table 2 for a list of excluded papers). Sixteen papers were included for analysis. Each of the 16 papers were assessed utilising the CCAT. Scores from the two independent appraisals were discussed and compared by the research team, with the average score for each paper outlined in Table 2. The independent scoring of each domain is also outlined in Table 2, providing a granular and transparent overview of the appraisal process. The total scores across the sixteen papers ranged from 68.75% to 87.5%, indicating satisfactory quality, with no papers excluded based on the CCAT score.
Table 2 Crowe Critical Appraisal Tool (CCAT) scores outlining the quality appraisal of included papersA total of sixteen papers were included in the review representing five high-income nations – the United States of America (n = 10), Australia (n = 3), Finland (n = 1), Norway (n = 1), and Israel (n = 1). The total number of participants represented in the papers is 963,718 of which 812,052 had a history of GDM and 151,666 did not. Fifteen papers used a quantitative design, and one used a qualitative design. The fifteen papers using a quantitative study design included: eleven cohort studies [43, 44, 46, 48, 49, 51,52,53,54, 56, 57]; two papers with both a cross-sectional and a cohort design [47, 55]; one prospective case control study [45]; and one randomised control trial [58]. Three papers used the US Infant Feeding Practices Study II data set [47, 49, 53] however, they reported on different aspects of it. Data collection methods varied between studies and included hospital records, birth registers, national statistics, and surveys. The single qualitative paper involved a phenomenological approach [50]. A summary of data extracted from the included papers is found in Table 3.
Table 3 Summary of included studiesThe findings from this review have been integrated and are presented under four broad themes, constructed during the analysis. The four broad themes are: breastfeeding outcomes, maternity care practices, maternal factors and family influences, and underlying determinants of health, and these findings are outlined in Table 4.
Breastfeeding outcomes
Ten quantitative studies reported on breastfeeding outcomes – initiation and duration [43, 44, 46, 49, 51,52,53,54,55, 57].
Initiation
Cordero et al. found the most significant predictor of breastfeeding initiation was intention of breastfeeding [46]. However, one study found women with a recent history of GDM were less likely to report breastfeeding in the first hour (aOR 0.83; 95% CI 0.73, 0.94); feeding on demand (0.86; 0.74, 0.99); and feeding only breast milk in the hospital (0.73; 0.65, 0.82) in comparison to women without GDM [57]. Two papers reported similar findings. Loewenberg Weisband et al. found women with GDM were had a lower likelihood of intending to exclusively breastfeed than women without GDM (aOR 0.71; 95% CI 0.51, 0.99) [53]. Similarly, Chamberlain et al. also reported that women with GDM were also less likely to exclusively breastfeed than women without GDM (OR 0.32; 95% CI 0.27, 0.38, P < 0.0001) [44].
Two studies found similar rates of breastfeeding initiation regardless of GDM status. Kachoria and Oza-Frank found predictors of breastfeeding initiation were mostly similar among mothers with GDM and those without [51]. Whilst Baerug et al. found that 99% of all women initiated breastfeeding regardless of GDM status [43]. However, after 12 weeks, only 56% of the mothers with GDM compared to 67% of the mothers without GDM predominantly breastfed (p = 0.02) [43].
Duration
Three studies reported that women with GDM were less likely to breastfeed on discharge. Haile et al. found that at hospital discharge, 62.2% among women with a recent history of GDM exclusively breastfed, compared to 75.4% of women without GDM (P < 0.01) [49]. Longmore et al. similarly found that 75% (OR 0.7; 95% CI 0.4, 1.3) of women with GDM breastfed on discharge compared to 84% of women without GDM [54]. Morrison et al. found that while 97% of women with a recent history of GDM had ‘ever’ breastfeed, only 19% had breastfed for 3 months (p = 0.001) [55]. Two studies found there was no difference in the duration of breastfeeding when comparing women with GDM and those without GDM. Loewenberg Weisband et al. found that regardless of GDM, breastfeeding duration was similar when comparing exclusive breastfeeding intentions and by hospital supplementations [53]. Laine et al. also reported no differences in the duration of breastfeeding when comparing women with GDM (7.5 months [SD 3.7]) and those without GDM (7.9 months [SD 3.7]) (p = 0.17) [52].
Across the papers there were variations in the findings in relation to initiation and duration of breastfeeding. Women with GDM may be just as likely to initiate breastfeeding as women without GDM, however, across the studies, it appeared women with GDM were more likely to report delays to breastfeeding in the first hour, were less likely to exclusively breastfeed or were more likely to cease breastfeeding than women without GDM.
Maternity care practices
Eight quantitative studies and the qualitative study reported on maternity care practices which influenced breastfeeding outcomes, these are largely birth interventions and complications, supplementation with CMF, and education and support [44, 46,47,48, 50, 55,56,57,58].
Birth interventions and complications
Birth interventions and complications after a pregnancy affected by GDM were associated with an increased risk of maternal-infant separation. Doughty et al. found that for women with GDM, newborns were less likely to stay with them in their hospital room than women without GDM (aOR 0.55; 95% CI 0.36, 0.85) [47]. Risk factors for not initiating or breastfeeding less than 30 days included infants with a health problem or prematurity [46]. Morrison et al. [55] describe an association between caesarean birth and the cessation of breastfeeding before 3 months (OR 1.70; 95% CI 1.04, 2.76) [55]. Similarly, Chamberlain et al. [44] reported lower breastfeeding rates among women having a preterm infant or caesarean birth [44]. Maternal-infant separation following birth was reported to affect breastfeeding, milk supply and bonding as one woman explains:
“They let me see him for just a second and then they said that he needed to go to the nursery for monitoring. . . I didn’t get him skin to skin for hours” [50]
Supplementation with CMF
Several papers reported on the use of CMF for women with GDM. Oza-Frank et al. [56] reported an increasing trend of women with a recent history of GDM being offered CMF as a strategy to address any breastfeeding challenges [56]. They found women with a recent history of GDM were more likely to introduce commercial milk formula (CMF) within the first two days (79.4%), than women without GDM (53.8%) (P < 0.01; aOR 3.48; 95% CI 1.47, 8.26) [56]. Oza-Frank et al. found women with a recent history of GDM were more likely to receive a pump (OR 1.28; 95% CI 1.07, 1.53) and a CMF gift-pack (OR 1.17; 95% CI 1.03, 1.34) compared with women without GDM [57]. Women with GDM were more likely to report that their physicians prefer CMF (aOR 2.82; 95% CI 1.17, 6.79) [47]. Jagiello and Azulay Chertok reported that the rate of CMF use during hospital stays where there was no medical indication was 68.4% (n = 39) [50]. The indication for the use of CMF was neonatal hypoglycaemia, along with other medical conditions. However, hospital records showed that CMF was given to these infants, even though it was not medically indicated [50].
Jagiello and Azulay Chertok found some women felt under supported by their maternity care providers and felt encouraged to supplement with CMF [50]:
“The nurses in the hospital insisted on giving formula. Now the baby is not satisfied with breastfeeding and I am not sure that I have enough milk so I start with breastfeeding and then give formula.” [50]
“I was pretty traumatized at day four when I went to the pediatrician and they threw some formula at me and said . . . put your baby on formula because you’re not giving him enough.” [50]
Education and support
Consistent support and advice was described as important to promote breastfeeding. Stuebe et al. found women with a recent history of GDM who received specialised breastfeeding education were less likely to stop breastfeeding (aHR 0.40; 95% CI 0.21, 0.74), or to introduce CMF (aHR 0.50; 95% CI 0.34, 0.72), than women with a recent history of GDM who did not receive the specialised education [58]. Griffin et al. found that women who had received an International Board-Certified Lactation Consultant (IBCLC) consultation were more likely to report ‘any’ breastfeeding on discharge (aOR 4.87; 95% CI 2.67, 8.86) and at 3 months postpartum (aOR 5.39; 95% CI 2.61, 11.16), compared to women who did not receive this consultation [48]. Jagiello and Azulay Chertok report the support of lactation consultations being highly valued in providing education, strategies, and advice to provide reassurance and address breastfeeding challenges [50]. As one woman describes:
“[She] changed everything for me. When she came . . . and my mom was like . . . she’s worth her weight in gold.” [50]
Women with GDM are more likely to experience delayed contact with their infants and are more likely to be encouraged to supplement with CMF. However, with appropriate and timely education and support, women with GDM can experience successful breastfeeding outcomes.
Maternal factors and family influences
Seven quantitative studies and the qualitative study reported on maternal factors and family influences on breastfeeding [45,46,47, 49,50,51,52, 55].
Maternal factors
Chertok and Sherby found a significantly greater proportion of women with a recent history of GDM reported perceived delayed lactogenesis II compared with women without DM (Fisher’s exact test, p = 0.029) [45]. Whilst Jagiello and Azulay Chertok revealed that 41% of women in their study reported delayed lactogenesis II and 44% reported perceived insufficient milk supply [50]. A perception of insufficient milk supply was described by women as frustrating and feeling as though they were depriving their infant of nourishment [50]. Concerns for the infant’s health following birth also influenced breastfeeding. Among the infants in their study, 33.3% (n = 9) had experienced complications including hypoglycaemia (14.8%, n = 4) [50].
One large quantitative study [51] retrospectively reported that mothers who were overweight with a history of GDM were as likely to breastfeed as women with GDM without overweight (OR 0.95; 95% CI 0.87, 1.03) [51]. However, a lack of specific data on breastfeeding practices reduces confidence in the findings. Similar findings were reported by Haile et al. [49] with no statistical difference found between women who had normal gestational weight gain and women who exceeded the recommended guidelines [49]. However, Haile et al. [49] found that women who had gestational weight gain below the Institute of Medicine guidelines, were less likely to exclusively breastfeed in comparison to women who experienced normal gestational weight gain (OR 0.62; 95% CI 0.45, 0.85) [49].
Conversely, two studies found a greater body mass index (BMI) was associated with breastfeeding outcomes that do not meet the well-documented WHO guidelines [59]. Morrison et al. found that a higher BMI (2 unit increased) was associated with cessation of breastfeeding at or before 3 months (OR 1.08; 95% CI 1.01, 1.57) [55]. Similarly, Laine et al. found women who breastfed for less than 6 months had a higher pre-pregnancy BMI than women who breastfed for 6 months or longer (P < 0.001 for linearity) [52]. Cordero et al. also reported that being overweight or severely obese increased the likelihood of not breastfeeding at 30 days. This finding was associated with smoking during pregnancy and having a caesarean section [46].
Family influences
Morrison et al. found that breastfeeding problems at home was association with cessation of breastfeeding at or before 3 months (aOR 8.01; 95% CI 4.57, 14.05); returning to work within the first three months (OR 3.39; 95% CI 1.53, 7.55), and women experiencing inadequate breastfeeding support (OR 1.88; 95% CI 1.10, 3.22) [55]. However, Morrison et al. reported being in a de facto relationship or married was a protective factor against the early cessation of breastfeeding (OR 0.14; 95% CI 0.03, 0.62) [55]. Partner, family, and friend support were cited as supportive resources [50]:
“My husband’s awesome . . . he’s like, [you should breastfeed] because it’s healthier for him and it’s healthier for you.” [50]
Jagiello and Azulay Chertok found some women were encouraged to terminate breastfeeding and/or supplement with formula following breastfeeding challenges such as delayed lactogenesis or decreased milk supply [50].
“and people are . . . like you should just stop, you should just pump, you should just use formula, why are you doing this?” [50]
Women with GDM are more likely to experience delayed lactogenesis II or perceived insufficient milk supply and more likely to experience breastfeeding challenges than women without GDM. However, breastfeeding success can be enhanced in women with a supportive network and encouragement.
Determinants of health
It appears that there are several determinants of health influencing breastfeeding outcomes and creating an added barrier for women with a history of GDM [43, 44, 46,





Comments (0)