
Remember me
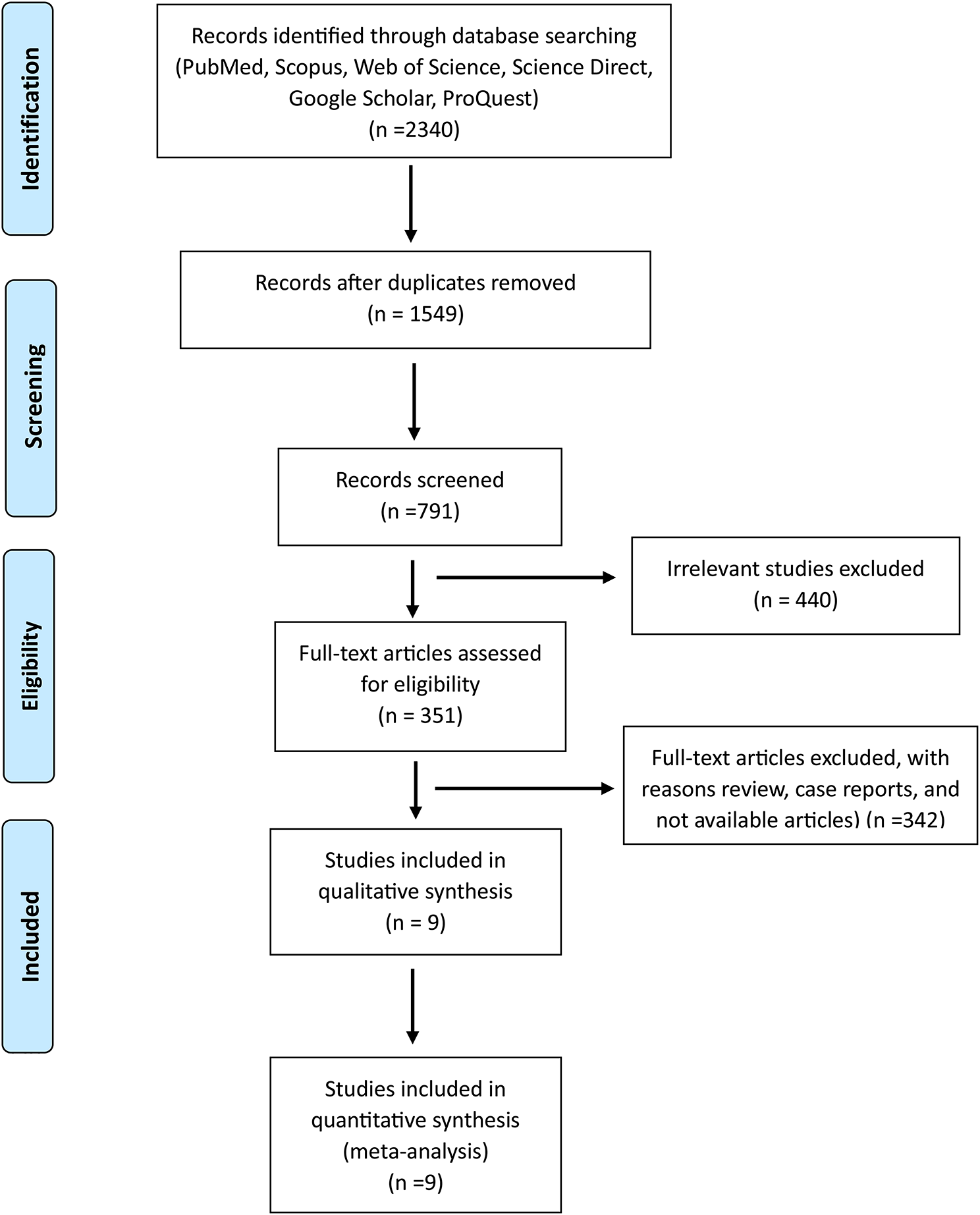




A total of 18 research articles comprising 991 patients were included in this review. Although 19 studies (with a total of 1136 patients) met the inclusion and exclusion criteria, all aggregate values and percentages were based on 18 studies (i.e., one was excluded). This was because 2 studies that were performed by the same lead author utilized the same patient population, which they alternately described as a cohort versus a cross-sectional/diagnostic accuracy study.
As illustrated in Fig. 2, the majority of papers were from Egypt, followed by South Africa. The majority (88.89%) of prospective endometrial cancer research in Africa was from North Africa, with Egypt encompassing 83.33% of all papers. Most of these studies focused on advanced imaging modalities. Research on the treatment of endometrial cancer is still emerging, with only one-third of the reviewed publications addressing it and 67% being diagnostic related. Of all the included articles, only 11.11% represented Sub-Saharan Africa, all from South Africa. While the average Human Development Index (HDI) in Africa is 0.536 [25], the average HDI of the represented countries in this study was 0.709 (min 0.707, max 0.740). The three countries represented, Egypt, South Africa, and Tunisia, all had high HDIs of 0.707, 0.709, and 0.740, respectively.
Fig. 2
Geographic Distribution of Prospective Endometrial Cancer Research within Africa. The map represents individual countries only and does not clearly illustrate some of the smaller African countries
There has been an increase in the number of studies published recently, with 50.01% of papers having been published from 2019 to 2021 compared with 27.7% of papers from 2010 to 2013 and 22.2% from 2015 to 2018. Although these studies were mostly designed as cohort studies (61.11%), cross-sectional studies and randomized controlled trials were the second- and third-most common study designs (both 11.1%). All but one study was performed at a single center (94.5%). Only 16.67% of studies had confirmed funding sources, 33.33% were unfunded and 49.96% had unknown funding. The majority (89.4%) of studies were performed in the university setting. The remaining population was equally divided between an oncology institute setting (5.56%) and the urban setting of Soweto (5.56%).
There were a total of 991 patients in these studies. For studies that reported age of diagnosis (n = 15, 83.3%), there was no consensus method of reporting age, with 12 studies (66.7%) reporting age ranges for a cumulative range of 31–81 years old. Thirteen studies (72.2%) reported the mean age with an average of 57.97 years old (min 49.5, max 66.4) across all studies, and 4 studies (22.2%) reported the median age with an average of 59.25 years old (min 58, max 60) across all studies. Three out of 4 studies reporting median age had a median age < 60 years old. The majority of studies (n = 8, 44.4%) reported mean age at diagnosis to be < 60 years old compared with “mean age ≥ 60” and “unknown mean age” each at 27.7% (n = 5).
Although multiple articles included multiple histologies of endometrial cancer, most articles addressed endometroid adenocarcinoma (n = 13, 72.2%) and serous/papillary serous carcinoma (n = 6, 33.3%). Molecular classification was not well documented in all studies. Data on stage distribution were only reported in 7 studies (38.9%), and all these studies were from Egypt. Similarly, survival probability data were available for only 4 studies (22.2%), all from Egypt.
Critical appraisal of study quality & bias, performed using the appropriate bias tools for each study design (see Tables 2, 3 below), showed that apart from the randomized controlled trials, all other studies were scored as either “fair” or “good” quality when translated to AHRQ standards. Case‒control and cross-sectional studies with a range of 7–8 points were scored as “Good” studies, with each study attaining “3 or 4 stars in the selection domain AND 1 or 2 stars in the comparability domain AND 2 or 3 stars in the outcome/exposure domain” [23]. The cohort studies, with a range of 7–9 points, were scored as either “Good” (n = 8) or “Fair” (n = 4) studies, with the majority of studies attaining “3 or 4 stars in the selection domain AND 1 or 2 stars in the comparability domain AND 2 or 3 stars in the outcome/exposure domain” [23]. Cohort studies scored as “Fair”, either had deficiency in the selection or comparability domains. The two randomized controlled trials were scored as “High risk of bias” and “Some concerns”, respectively, due in large part to deficiencies in the “Outcome” and “Reporting” sections, suggesting a need for improvement of these sections during the study-planning phase.
Table 3 Results of critical appraisal of included observational studies using Newcastle‒Ottawa scores
Comments (0)