TFCC injury is a frequent soft tissue injury that has been observed to accompany distal radius fractures, which are rather common. The Palmer’s classification method states that TFCC injury of Palmer type IB is known to lead to instability of the DRUJ [17, 18]. In addition, instability of the DRUJ can lead to early onset of arthritis, decreased grip strength, a restriction of the range of motion (ROM) of the wrist joint, and persistent discomfort in the wrist if it is not properly treated. It is also recognized as a factor with a poor outcome for distal radius fractures [19]. Distal radius radiographs are utilized for diagnosis, treatment planning, fracture reduction evaluation, and healing monitoring. If these radiographic characteristics could help us determine whether a fracture has occurred while also initially determining whether the TFCC is injured or not, that would be very significant.
Our investigation showed that traumatic TFCC injury occurred in 54.1% of patients with DRF (75.6% in C3 type). 1B TFCC injury was most common, with an incidence of 26.7% in all patients with DRF and 49.5% (table not shown) in the TFCC injury group. Moreover, the general radius length and DRUJ distance of the TFCC injury group were 4.83 mm and 2.95 mm, respectively. A shorter radius length was related to lB TFCC injury. Radius length and DRUJ distance cannot be utilized as predictors even if they have a statistical correlation with TFCC injury.
Studies are conflicting regarding the relationship between traumatic TFCC injury and radiologic parameters in patients with DRF. K. Kasapinova et al. [20] noted that the initial radiograph of a distal radius fracture does not predict a triangular fibrocartilage complex injury. In contrast, Beom-Soo et al. [21] mentioned that the shortening of the distal radius, causing peripheral soft tissue of the ulnar side to become tauter, is highly relevant with regard to the pattern of TFCC injury. However, in those studies, relatively little clinical data were collected. This study has the most numerous strengths in that it collected complete imaging data, including X-ray, CT, and MRI from 172 patients, and identified the relationship between radius length as well as DRUJ distance and TFCC injury through imaging modalities. Moreover, this study demonstrates that type 1B TFCC injuries are more common in distal radius fractures and that TFCC injuries are not necessarily the worst in intra-articular fractures; for example, the incidence of TFCC injury is higher in type B3 distal radius fractures than in C1 and C2 fractures.
Distal radius fracture displacing more than 4 mm and tilt radially beyond 0° and dorsally > 10° have significant clinical implications because distal radius fractures with shortening or dorsal tilt beyond the above values will influence DRUJ instability. As early as 1997, Richards et al. [9] found a relationship between the initial displacement of DRF and the presence of TFCC injury which was associated with significantly greater shortening and dorsal angulation of the radius compared with fractures where the TFCC was uninjured. Kwon et al. [22] reported that initial distal radial shortening of more than 6.0 mm is one of the risk factors for TFCC injury and DRUJ instability. Previous studies have shown that an increase in DRUJ distance is an independent risk factor for DRUJ instability in distal radius fractures [7]. In addition, Omokawa et al. [23] reported that the DRUJ gap distance is the most important predictor of TFCC injury accompanying an unstable distal radius fracture. In this study, patients with TFCC injury tended to have a shortened radius and widened DRUJ distance, although they had no predictive value for TFCC injury in DRF. Prior research has shown a correlation between TFCC injury and the amount of dorsal or volar angulation in the fracture [24, 25]; however, there was no significant relationship between the palmer tilt angle and other radiologic parameters and TFCC injury in this study.
Since 1B TFCC injury may result in DRUJ instability, some researchers advised treating the TFCC injury if DRUJ instability is detected after the fixation of DRF [26]. However, DRUJ instability may not be reliably detected by manual stress tests, such as the radioulnar stress test [27, 28]. Perioperative manual stress testing, in particular, cannot effectively detect DRUJ instability because edema or subcutaneous hematoma around the wrists would make identification difficult. According to our research, a shorter radius length was associated with 1B TFCC injury and could serve as a significant reference value. Specifically, radial length of less than 5 mm following DRF was associated with a higher risk of 1B TFCC injury; however, a slight variation in radius length does not always mean the absence of TFCC injury. Although the significant instability of the DRUJ due to 1B TFCC injury would be the cause of the residual ulnar wrist pain, which type of 1B TFCC injury arouses the DRUJ instability which results in the residual symptoms are still unknown and further investigation should be needed.
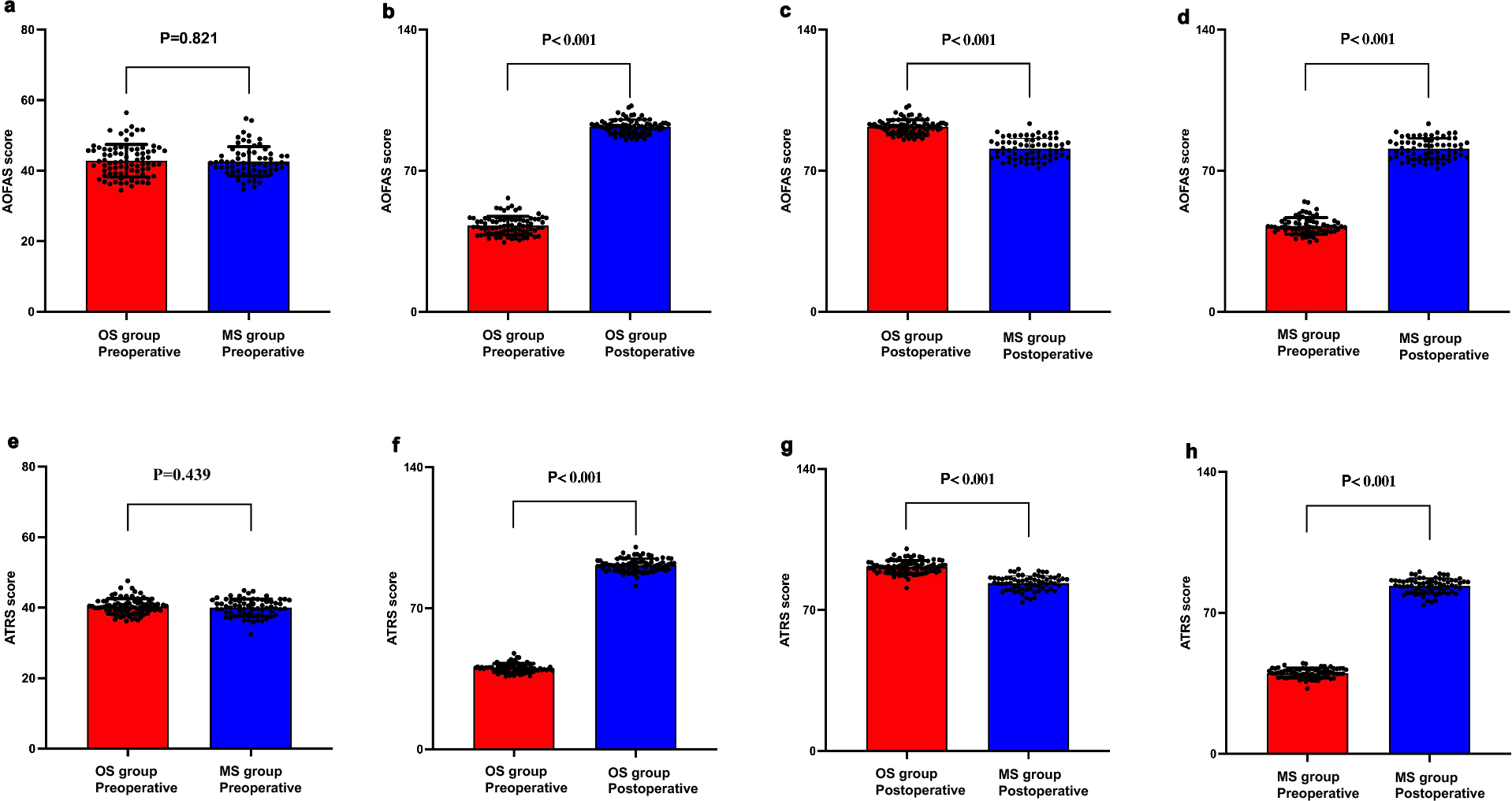
The treatment goals for DRF are painless and fully functional wrist motion. Although the treatment of DRF with VLP fixation reportedly achieves satisfactory outcomes, several researchers have reported that some patients experience ulnar wrist pain after surgical treatment of DRF [29]. TFCC injuries are a recognized cause of ulnar side wrist pain, resulting in unsatisfactory outcomes [5, 6]. Many authors have recommended surgical repair of the TFCC in distal radius fractures to prevent the adverse effect of instability of the DRUJ and ulnar side wrist pain [30]. In contrast, authors who recommend conservative treatment have reported that long-arm splinting for 1 month after internal fixation of the distal radius fracture with instability of the DRUJ could result in a satisfactory outcome [31]. Moreover, Jemin et al. [32] found that there were no statistically significant differences in the clinical outcomes between surgical and conservative treatment. Although controversial, we must treat TFCC injury with the proper treatment methods to minimize their negative effects on the patient as much as possible. In clinical practice, it is possible to select a customized treatment plan following appropriate patient discussion. Even though the majority of patients choose a conservative course of therapy, the surgeon should still be well-informed on the current debates surrounding the management of TFCC injury as well as the potential postoperative consequences. The height of the radius should be restored as much as possible during surgery in cases with DRF with substantial shortening of the radius (particularly if the radius length is less than 5 mm). Furthermore, it is recommended to use a wrist brace or splinting for 4 to 6 weeks to fix the wrist in order to prevent TFCC injury and potential DRUJ instability. Still, further investigation is required as this is only the researchers’ observation.
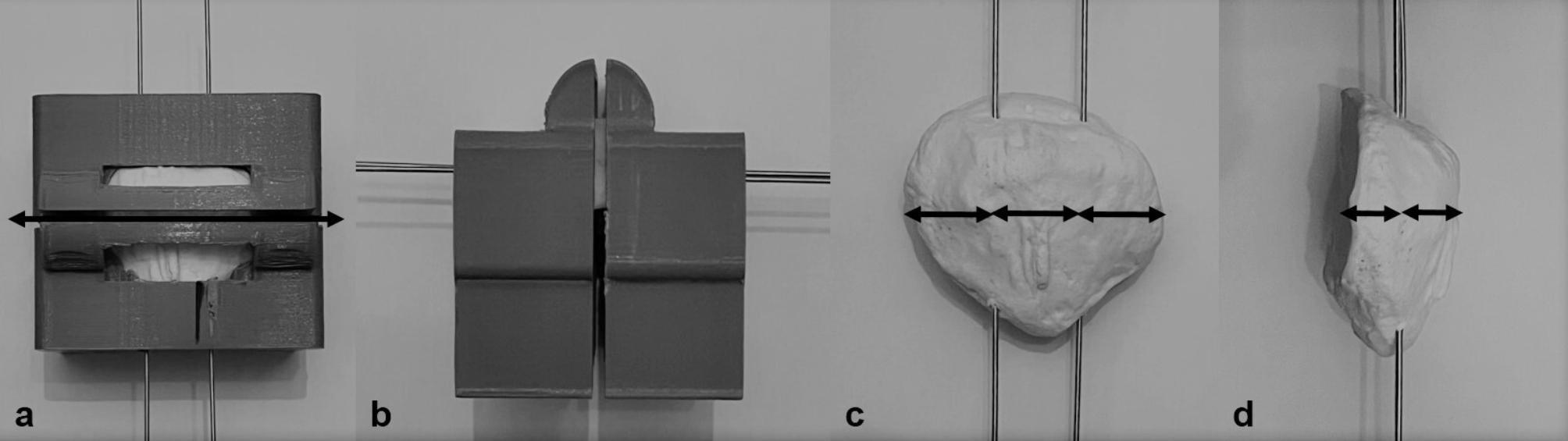
There are a few limitations to this study. The main limitation is in the measurement and categorization of the relevant image data. This study involves a large number of radiologic parameters, and measurement on X-ray is prone to bias, but it is truly the most straightforward and constrained approach available. Measurement by CT may be more accurate, but there are many problems in practice, such as the measurement of angles. The classification of TFCC injury by analyzing MRI is also subjective, and perhaps the results would be more accurate afterward with arthroscopy. Another limitation is that this study focused on radiologic parameters and ignored the influence of other factors on TFCC injury, such as ulnar styloid fracture, which may have some relevance to TFCC injury [33, 34]. Therefore, further investigation of the differences in the clinical outcomes of distal radius fractures is needed.









Comments (0)