
Remember me




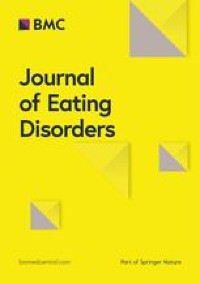

We identified the following two main themes related to patients’ experiences with BED (Fig. 1): (1) A challenging addiction with the subthemes giving it a name, living in a negative spiral and it’s in your head; and (2) shame with the subthemes painful thoughts and feelings, negative self-image and feeling misunderstood. We found three main themes regarding the perceived facilitators of recovery: (1) recovery is a long process with the subthemes acceptance of the disorder and give yourself time; (2) coping with the subthemes self-compassion and strategies to manage the disorder; (3) community with the subthemes group affiliation and social support.
Fig. 1
Main themes and subthemes concerning the experience of living with BED
Experiences of living with BEDThe participants described living with BED as a challenging addiction. Berit explained how difficult it was to stop eating: ‘When I eat, I get happy right there and then, but when I think about it, and the dopamine or whatever it is stops working, I feel completely unsuccessful, and then I think that I can just give up. It is over. I just continue to eat. … I can’t do anything right anyway’.
Giving it a name describes participants’ experienced relief of being diagnosed with BED. The participants experienced BED as a complex condition and a challenging disorder that removed their focus from other notable areas of life. They often told stories of repeated feelings of failure in their management of BED. They felt too embarrassed to tell anyone in their lives about their diagnoses and, thus, kept it a secret, even though they thought their family members already probably knew. Their frustration with not being able to control their eating was described as confusing and time consuming. They felt hopeless and stupid. However, being diagnosed with BED was often described as a relief, which Nora expressed:
‘It’s actually been really nice. (...) I was referred because of my overweight, uhh, and based on mapping and such, I was diagnosed with binge eating disorder. And I was about to say, uhh, that I wasn’t completely surprised. I’ve realised in a way that there has been a problem, uhh, but at the same time, it was kind of good to have it confirmed (...)’.
All participants were diagnosed with BED at the rehabilitation centre.
The participants described living with BED as a negative spiral that was difficult to escape and characterised by periods of guilt when they could not control their eating habits. Tuva explained, ‘Yes, it’s like I don’t use my head. I don’t do what I’m supposed to, ehh, and I don’t enjoy it. I sit and eat with a guilty conscience’. Conversely, the participants stated that binging gave them good feelings and satisfaction. These binge eating episodes were considered a reward or a strategy to escape stressful experiences in daily life.
Dealing with binge eating was often viewed in the context of how they otherwise felt in life. A negative spiral was also mentioned concerning weight management experiences. Individuals had experiences in which they lost weight but had trouble maintaining weight loss. This led to dissatisfaction and hopelessness and resulted in episodes of increased binge eating. Some participants had lived with BED for a long time and had experienced BED as a permanent part of them.
Participants experienced BED as something that is in your head, as Pia expressed: ‘At least it starts there, that the body is a symptom of what’s in the head. I think that about my suffering, that the physical kind of reflects the mental’. It was vital for participants to understand the connection between physical and mental challenges and how these affect each other. Negative thoughts and feelings often led to binge eating episodes, and subjects appreciated the focus on mental health in the rehabilitation centre to learn strategies to cope and choose differently.
All participants associated BED with shame, as illustrated by Berit’s statement:
‘It is very taboo, very taboo. I try to hide it from everyone. When we’re with others, I don’t eat more than others, but when I’m at home and no one sees me, that’s when I eat. So, it’s tiring, and you always watch out. You never feel well enough, and uhh yeah, it really hurts’. Shame was often described as painful feelings and negative thoughts. The participants often felt ashamed when other people asked them, ‘Why can’t you just stop eating?’ This question made them feel ashamed of not being in control of their eating behaviours. In this context, the respondents explained that most binge eating episodes occurred when they were alone to avoid feelings of shame. The participants had many negative thoughts and spent much time ruminating about what others thought about them. Thus, shame often related to subjects’ negative self-image, as this comment by Pia illustrated: ‘That’s kind of what the body ideals are today, thin and slim, and if you don’t fit in that category, there’s something wrong with you’.
Several participants described having a negative self-image and critical thoughts about their bodies and behaviours. They mentioned that they already had negative self-images before developing obesity and being diagnosed with BED. Obesity was considered challenging in terms of physical limitations and mental health struggles. They described feelings of not fitting into the bodily ideals in today’s society, where thinness and health are expected.
Living with shame was also connected to a feeling of being misunderstood by family members, friends or even health professionals. Berit stated: ‘I had a doctor who said, “You just have to pull yourself together. You just have to eat right”. I think there are probably a lot of doctors who don’t have knowledge about binge eating’.
Participants experienced little openness about BED. They expressed that they feel it is more common to talk and hear about anorexia and bulimia. Having a less-known eating disorder makes it harder to be open and honest. Some kept the disorder a secret from family and friends, which again worsened their shame and hopelessness.
Facilitators of recovery processesRecovery from BED was often considered a long process involving accepting the disorder and giving oneself time. Participants defined ‘recovery’ as the process of reducing binge eating and enhancing coping. Being healthy did not imply the total absence of binge eating episodes, but having greater control over the occurrence and amount of food consumed during binge eating episodes, as Kari explained: ‘It is about coping with it so that it does not happen so often and regularly, but to accept that it can happen once in a while and that it is normal and that you should not feel that you have failed. Because I think that when it happens once, seldom, that I have succeeded in recovering’. The participants did not perceive recovery from BED as being healthy, since they often had other diseases that they had to handle, such as diabetes.
They perceived it as important to have strategies to manage recovery, as Pia described: ‘I think that you have to work on it continuously. But I see a change because I have gotten some tools that I can use in such situations, and I have another mindset now. I feel more relaxed’.
Managing to cope with recurring binge eating episodes was considered an important facilitator of recovery. Participants associated coping with exerting control over their eating behaviours. Many subjects felt more in control with others but felt they could lose it when they were alone, as Silje explained: ‘It’s kind of like how you compare yourself to others and how they manage to control their eating, uhh, and that's what I want, too’.
The participants often managed to have control by avoiding access to foods that triggered BED (e.g. sweets). Nora said, ‘I have the knowledge to choose the food that’s right for me, and I need to have it available’. Furthermore, they related coping to ‘inner factors’ that influence their health and quality of life. For instance, focusing on health aspects was considered more important than focusing on weight. Health aspects were also an important motivation for recovery. Several participants explained that pain due to being overweight, such as knee arthrosis, motivated them to control their BED.
In addition, self-compassion was often mentioned as a significant facilitator of recovery. Participants gave themselves credit and bragged about periods without binge eating as positively self-reinforcing, often disrupting their negative spirals. Pia explained, ‘Self-compassion is very important for me, hm, being good with myself, being my own best friend and to think about what is good for me. Like, ‘Are episodes with binge eating good for me? No, they are not. It is better for me to go for a walk or to eat fruit’. However, the participants said that self-compassion requires awareness and practice. They highlighted getting older, gaining life experience and being more mature and reflective as factors that made it easier to give oneself acceptance.
‘Time outs’ from eating were reported as an important strategy to manage the disorder. The patients stated that breaks gave them time to reflect on why they were eating, as Berit explained: ‘It has also helped me to wait for 15 min and to eat what you like. Take a 15-min break to see if I really want to eat. Very often, you actually don’t want to. I may start to eat, but then I am at least more aware of eating.’ Another participant stated that it was important not to be too strict with oneself and not to have overly strict rules, such as ‘yes food’ and ‘no food’, to cope with BED. Good eating routines were another factor that facilitated recovery. Outdoor activities, listening to music, reading books, knitting and talking to oneself often helped interviewees to avoid new BED episodes. They appreciated that the present rehabilitation programme focused on mental health, well-being and personal relationships with food. Learning about BED gave them a better understanding that obesity did not just result from a lack of self-control and willpower.
One of the most significant facilitators for managing recovery was a community characterised by group affiliation and social support. All outlined the importance of the community at the rehabilitation centre, as Pia described: ‘It was very good to meet others in the same situation and to get validation that there are more people in the same situation and that you can talk to them openly about these episodes without being judged’.
Some participants feared how they would cope with BED once they no longer belonged to a rehabilitation programme. The perceived social support of others in the group gave them safety. Nora explained, ‘It was very good to not feel alone (…) to hear that others have the same problems. This made it easier to share my experiences. Being together with others in the same situation makes me feel safe’. The subjects learned to share BED-related experiences and feelings in the group. For recovery, they also considered it important to learn to share their feelings with others outside the programme, as Nora said: ‘I have been better about talking about my feelings at home, for example “Now I am alone, and I am sad because you are not here”’.
Comments (0)