
Remember me



With a prevalence of 1%–2% (1), celiac disease (CD) is one of childhood’s most common chronic diseases. In CD, gluten ingestion causes an immune reaction leading to small intestinal inflammation and villous atrophy. It can lead to gastrointestinal and extra-intestinal symptoms, including poor growth in children (2). A strict gluten-free diet (GFD) is the only effective treatment for CD (3). However, such a strict diet may be difficult to sustain and could lead to social difficulties, especially during adolescence (4). CD has been linked to reduced health-related quality of life (HRQoL), albeit inconsistently (5–13).
Clinical follow-up of CD aims to ensure a strict GFD, monitor symptoms, and prevent disease-related complications (14). Previously, we, and others have reported a lack of follow-up in 14%–57% of celiac children and young adults (15–17). However, few studies have examined the association between the lack of follow-up and clinical outcomes (such as dietary adherence, disease remission status, and HRQoL). The only previous pediatric study in this field compared the dietary adherence and serologically defined remission rates between 50 Israeli children without follow-up and 52 children with continued follow-up for CD (18). The authors found dietary adherence rates and serologically defined remission to be much worse in patients without follow-up (18).
We tested the hypothesis that children who lack follow-up would have a poorer dietary adherence level, achieve disease remission to a lesser extent, and have poorer HRQoL than children with continued CD follow-up.
METHODSIn a cohort of 162 school-aged children with CD, we examined the association between the lack of follow-up versus continued follow-up and outcomes of dietary adherence level, disease remission status, and HRQoL using data from blood samples, patient charts, and validated questionnaires.
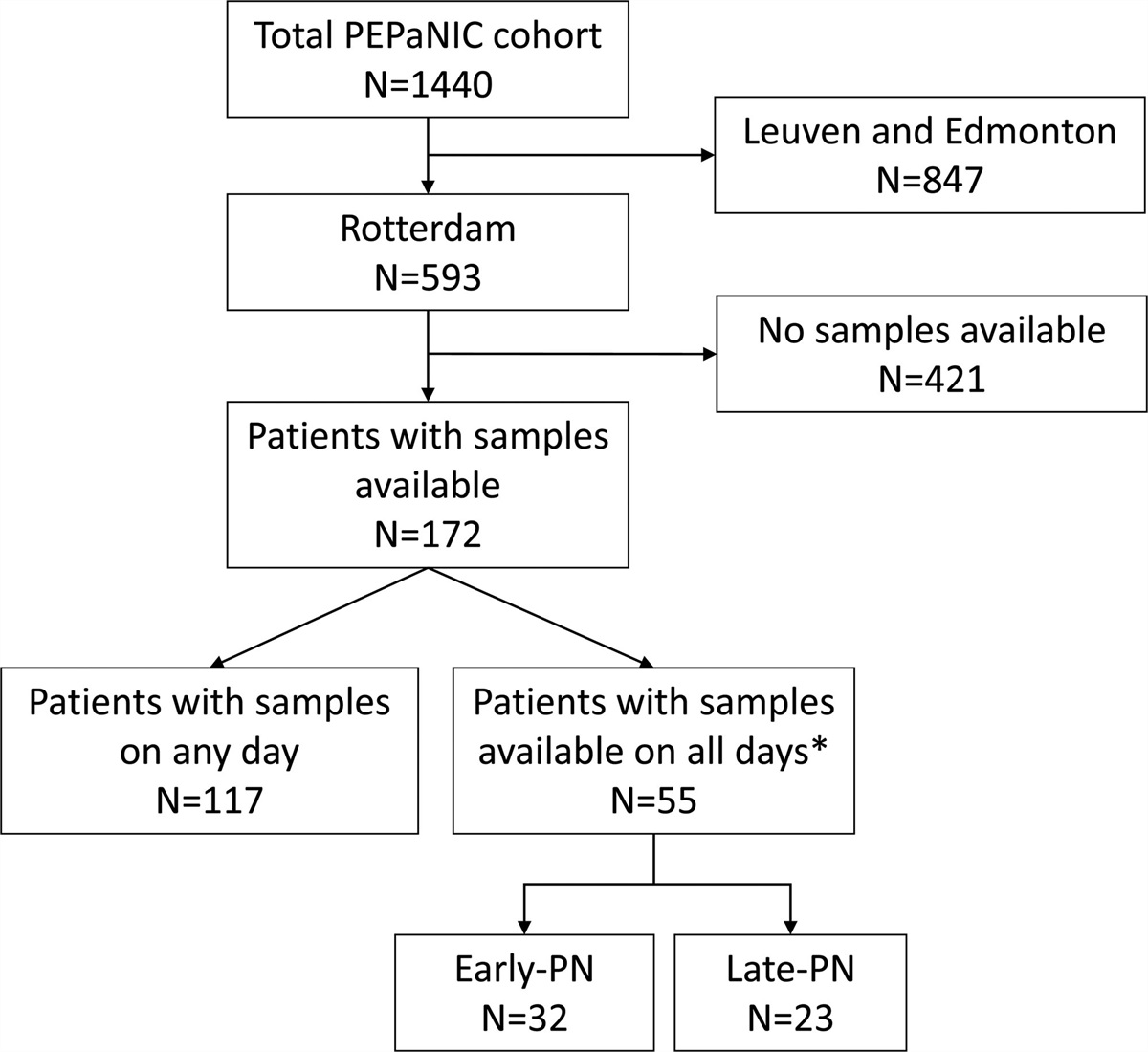
Study Setting and Sample PopulationBased on a previously described CD cohort (15), this study included 162 children diagnosed with CD in 2013–2018 at Queen Silvia Children’s Hospital, Sahlgrenska University Hospital, Gothenburg, Sweden. From 2013 to 2018 local guidelines required all pediatric CD in the Gothenburg metropolitan area to be diagnosed at Queen Silvia Children’s Hospital. After diagnosis, however, guidelines recommended CD follow-up at general pediatric outpatient clinics (exceptions included children with co-occurring type 1 diabetes cared for by pediatric endocrinologists).
Details of this celiac cohort’s formation and clinical follow-up practice have been presented elsewhere, and in Figure 1, Supplemental Digital Content 1, https://links.lww.com/MPG/D264 (15). In brief, of all 8–18-year-old children (n = 484) in the Gothenburg metropolitan area with at least 1 International Classification of Diseases code (K90.0) for CD, 336 (69%) had an established CD diagnosis according to the guidelines presented below. Of the 336 children with confirmed CD, stratified by calendar year of diagnosis 2013–2018, we randomly selected 243 (72%) to participate in the study. After obtaining informed consent, 162 (67%) participants were enrolled in the study between January and June 2021.
Diagnostic Definition of CDAccording to the Swedish version of the 2012 European Society for Paediatric Gastroenterology Hepatology and Nutrition guidelines (19), CD diagnoses for this study either required a small intestinal biopsy or repeatedly positive tissue-transglutaminase antibodies (tTGA). The biopsy approach needed crypt hyperplasia or villous atrophy with intraepithelial lymphocytosis (Marsh 2–3) (20). Diagnoses made using a non-biopsy approach required gastrointestinal symptoms (2,19), permissive human leucocyte antigen haplotypes, and repeated tTGA-Immunoglobulin A (IgA) 10 times the upper limit of normal (ie, ≥70 U/mL) (21). Endomysial antibody tests were not required because of the unavailability of these tests in Sweden (21). The time of CD diagnosis was defined as the diagnostic biopsy or, in non-biopsy verified CD, when patients were informed of their diagnosis. Through a patient chart review (15), we compiled results of diagnostic serology tests and biopsies.
Definition of the Lack of Follow-UpMotivated by recent consensus guidelines on CD follow-up (14), we defined the lack of follow-up as no documented visit for CD (physician or dietician) or tTGA measurement over the past 24 months of study enrolment. Data were recovered from patient charts and laboratory records.
Measurement of tTGAA blood draw was retrieved after study entry and analyzed for tTGA using a fluorescent enzyme immunoassay (Phadia AB, Uppsala, Sweden) at the Department of Clinic Immunology, Sahlgrenska University Hospital (Gothenburg, Sweden). For 10 children with a tTGA measurement recorded within 30 days of study enrolment, we used this result and did not require a repeated blood draw. All samples were tested for total IgA in addition to tTGA and in case of low IgA levels (<0.07 g/L), analyzed for IgG-type tTGA (n = 2). Motivated by a previous study (18), we defined disease remission as having a normalized tTGA (<7 U/mL).
Questionnaire DataWe administered all questionnaires through an electronic case report form (eCRF) (Medicase AB, Gothenburg, Sweden). Additional to the sociodemographic data provided by the parents, we encouraged the children to answer the questionnaires alone or with the assistance of their parents if needed. As described below, all questionnaires were administered at study enrollment without prior knowledge of patient follow-up practice.
Background CharacteristicsBriefly, we collected data on the responding parent’s age, education level (secondary school, university/college 0–3 years, or >4 years), employment (employed, sick leave/unemployed, student/parental leave), and country of birth (Sweden, Europe, Other) (Table 1) and parental cohabitation. Moreover, we obtained data on the children’s previous and current medical history, and first-degree heredity of chronic autoimmune diseases (eg, thyroid disease, type 1 diabetes) (15).
TABLE 1. - Background characteristics of children with lack of follow-up versus continued follow-up for celiac disease (CD) VariableLack of follow-up was defined as no registered visit for CD or tTGA over the past 24 months of study enrolment. SD = standard deviation; tTGA = tissue-transglutaminase antibodies.
*The parent who filled out the survey.
†Both parents.
‡Other diseases included renal or urinary tract disease, anemia, epileptic seizures, headache, neuropsychiatric disorders, overweight/obesity, congenital syndrome, psychiatric disorders, rheumatic disease, thyroid disease, type 1 diabetes, and developmental delay.
§Symptoms of CD, for example, abdominal pain, constipation.
∥First-degree relatives with CD.
¶CD screening due to type 1 diabetes.
#Including 10 children with a tTGA measurement recorded within 30 days of study enrolment.
We used the Swedish version of the Celiac Dietary Adherence Test (CDAT) to assess GFD adherence (22,23). In CDAT, an additive score was calculated from 7 items on a 5-point Likert scale. Scores <13 indicate very good adherence, scores >17 indicate poor adherence, and scores between 13 and 17 are considered inconclusive (22). CDAT has been validated for adults but has also been used in children aged ≥12 years (22,23).
SymptomsWe assessed the occurrence and severity of current gastrointestinal symptoms using the Gastrointestinal Symptom Rating Scale (GSRS) (24). This scale contains 15 items rated on a 7-point Likert scale. The 15 items are divided into 5 domains: “Diarrhea,” “Indigestion,” “Constipation,” “Abdominal pain,” and “Reflux.” In the GSRS a total score was calculated from all 15 items, as well as a mean score for each domain. Higher scores indicate more severe symptoms (24,25). While the GSRS was not explicitly designed for CD, it has been widely used in CD research, including in children (26–28).
We selected 3 items from the Celiac Symptom Index to identify extra-intestinal symptoms of CD: headache, reduced energy, and loss of appetite. These questions evaluated the frequency of CD-related symptoms over the past 4 weeks with a 5-point Likert scale from “none” to “all of the time” (29).
GrowthBased on parental reports, we collected information on the children’s height (cm) and weight (kg). The children’s weight and height were standardized according to growth data from the Swedish general population (30).
HRQoLKIDSCREEN-27 is a generic HRQoL instrument that has been extensively validated for children aged 8–18 years in many countries, including Sweden (31,32). The questionnaire addresses 5 dimensions of HRQoL: “Physical wellbeing,” “Psychological wellbeing,” “Autonomy and parent relations,” “Social support and peers,” and “School environment” (Methods 1, Supplemental Digital Content 2, https://links.lww.com/MPG/D265) (33).
We also evaluated CD-specific HRQoL using the Celiac Disease DUX (CDDUX), a 12-item questionnaire covering 3 dimensions: “Communication,” “Diet,” and “Having CD.” Dimension sub-scores and a total score were calculated and interpreted as very bad, bad, neutral, good, or excellent CD-related quality of life (34). The instrument has been validated for 8–18-year-olds (34–36).
Statistical AnalysesWe examined dietary adherence rate, tTGA levels, symptom scores, anthropometrics, and measures of HRQoL between children with versus without continued follow-up (ie, no follow-up for CD over the past 24 months).
For comparison between groups, Fisher exact test, the Mantel-Haenszel chi-square test, the chi-square test, and the Mann-Whitney U test were used as appropriate. Reported estimates are based on non-missing values, if not stated otherwise. Missingness was primarily due to incomplete answered questionnaires (as detailed in Tables 1–3).
After critical consideration of relevant literature we preselected the child’s sex, age, and parental education level as potential confounders between lack of follow-up and clinical outcome measures (eg, HRQoL). Then, using analysis of covariance, the following variables were added to the final model according to a >10% change between unadjusted and adjusted estimates: year of CD diagnosis, medical history, first-degree heredity for autoimmune diseases, and parental occupation (Table 1).
Post-Hoc Power AnalysisGiven a 5% significance level and a common standard deviation of 10.0 in both groups, we had 80% power to detect a minimum 6-point total score difference in KIDSCREEN-27 between children without follow-up (n = 23) versus children with continued follow-up (n = 139). Based on previous work (33), a 5-point total score difference was defined as the minimum clinically meaningful difference in KIDSCREEN-27 between groups.
SAS Version 9.4 (SAS Institute, Cary, USA) was used for the statistical analyses.
EthicsThis study was approved by the Swedish Ethical Review Authority (Dnr 2020-06033). For children 8–14 years, parental informed consent was obtained; for children 12–14 years, we also obtained the children’s assent to participate. Individual consent was obtained from children ≥15 years.
RESULTSIn this cohort of 162 children the average age was 12.7 years at study entry and a majority were girls; most children had been diagnosed using a non-biopsy approach (Table 1). The sociodemographic characteristics, medical history, and family history of chronic autoimmune diseases were similar between children with and without follow-up (Table 1). One in 7 celiac children had no CD-related visit or tTGA measurement over the past 24 months (classified as children without follow-up). Of these 23 non-followed-up children, 13 (56%) had a follow-up visit or tTGA measurement during the past 36 months. We received questionnaire data in 9 out of 10 participants. Ten children had, as part of their clinical follow-up, analyzed tTGA within 30 days of study entry and 107 (72%) provided a new blood sample for tTGA (Table 1).
Dietary Adherence and Disease RemissionSelf- or parent-reported data indicated a very good adherence to GFD (CDAT score <13) in most of children with and without continued follow-up. The distribution between very good, inconclusive, and poor adherence (CDAT score >17) was similar in children with versus without continued follow-up (P value = 0.41, Table 2).
TABLE 2. - Celiac Disease Adherence Test (CDAT) of children with lack of follow-up versus continued follow-up of celiac disease Continued follow-upn (% [95% CI])
Difference between groups adjusted means**The group means were adjusted for sex, age, year of CD diagnosis, medical history, first-degree heredity of autoimmune disease, parental occupation, and education level, and the difference between the adjusted means calculated. All P values > 0.4.
After a mean of 5.3 years since CD diagnosis (standard deviation 1.7, range 2.3–8.8), tTGA had normalized in 94% [n = 16; 95% confidence interval (CI): 71%–100%] of children without follow-up versus 91% (n = 91; 95% CI: 84%–96%) with continued follow-up. Figure 1 depicts the distribution of tTGA according to CD follow-up status.
 FIGURE 1.:
FIGURE 1.: Distribution of tissue transglutaminase antibodies (tTGA) in children with lack of follow-up versus continued follow-up for celiac disease (CD). Study-specific tTGA (n = 107), tTGA analyzed less than 30 days before study enrollment as part of regular follow-up (n = 10). tTGA level category: <7 [normal]; Positive (7–>100 U/mL); Positive (≥100 U/mL). Data stratified by patients with continued follow-up versus lack of follow-up (no CD-related physician/dietician-led counseling and prior tTGA measurement over the past 2 years [<24 months] of study enrollment).
Symptoms and GrowthUsing the GSRS, participants scored overall a low level of gastrointestinal symptoms (Table 3). We found similar total GSRS scores and comparable scores across its 5 dimensions for children without follow-up versus continued follow-up (all P values > 0.12, Table 3). Surveyed extra-intestinal symptoms of CD were also similar between the 2 groups of children (Table 3).
TABLE 3. - Gastrointestinal and extra-intestinal symptoms of celiac disease (CD) among children with lack of follow-up versus continued follow-up for CD Gastrointestinal Symptom Rating Scale (GSRS), mean (SD) Continued follow-upLack of follow-up was defined as no registered visit for CD or registered tissue transglutaminase antibodies over the past 24 months of study enrolment. Self/parent-reported gastrointestinal symptoms, measured with the Gastrointestinal Symptom Rating Scale (GSRS), where lower scores indicate less severe symptoms. The GSRS domain scores and total score range from 1 (no symptoms) to 7 (most severe). CI = confidence interval; SD = standard deviation.
*The group means were adjusted for sex, age, year of CD diagnosis, medical history, first-degree heredity of autoimmune disease, parental occupation, education level, and the difference between the adjusted means calculated.
†Frequency of extra-intestinal symptoms was related to the past 4 weeks and was measured using items from the Celiac symptom index (CSI) (24,29).‡All P values >0.15; all adjusted P values >0.10.
The average z score for weight was 0.1 (range, −4.7 to 3.2) for children with continued follow-up and −0.3 (range, −2.5 to 2.4) for those who lacked follow-up. Corresponding average z scores for height were 0.0 (−5.0 to 3.2) for children with follow-up and 0.0 (−1.5 to 2.4) for those who lacked continued follow-up (all P values > 0.17).
HRQoLChildren with and without follow-up for CD reported similar HRQoL to the standardized reference scores of KIDSCREEN-27. Over the 5 measured dimension scores and the total raw score, no significant between group differences were found (Table 1, Supplemental Digital Content 3, https://links.lww.com/MPG/D266). Moreover, both groups had similar CDDUX dimension scores and equal mean CDDUX total scores (CD-specific HRQoL).
DISCUSSIONUsing data from a regional cohort of 162 children with CD, this study compared outcomes in children without follow-up (ie, no CD-related consultation or tTGA measurement over the past 24 months) versus continued follow-up. There were no significant between-group differences in dietary adherence level, tTGA levels, symptoms, growth, or HRQoL. While our null-findings were seen in an overall minimally symptomatic group of children with a high rate of tTGA normalization, these results indicate that the frequency of CD follow-up visits may be adjusted to the individual’s need to achieve dietary adherence, symptom control, and normalization of CD-specific serology tests.
Interpretations of FindingsOur estimates of GFD adherence are consistent with a recent systematic review reporting median rates of GFD adherence between 75% and 87% of children (37). Previously, Barnea et al (18) have found a poorer level of GFD adherence, particularly in young adults and those without follow-up (almost half of whom consumed gluten deliberately) (18). By contrast, only 6% of our study cohort reported poor GFD adherence, and 71% reported very good GFD adherence.
Recent studies suggest that tTGA should normalize within 18–24 months after initiation of a GFD (14). Similar to other studies (38,39), >90% of the children in our cohort had normalized tTGA. We found no difference in tTGA levels between children with and those without follow-up of CD. This lack of difference contrasts with the results of Barnea et al (18), where 25% (n = 13/52) of their Israeli children with follow-up versus 50% (n = 25/50) without follow-up had not achieved serological normalization. While our results were based on tTGA measurements from recently collected blood samples, Barnea et al also included historic serology data (on average, almost 4 years old), and the type of CD-specific serology test was not reported. There are several differences between our study and previous works. For instance, ascertainment and incidences of CD vary widely by secular trends, as do the age and geographical region of the study population, and the access and means of CD follow-up. Other differences include the selection of patients under study and the definition of lack of follow-up. For instance, 1 previous study (18) included patients with potential CD, which may refer to a preclinical manifestation of the disease (40), and possibly a varying inclination to adhere to a GFD and follow-up. Previous works have defined lack of follow-up as “no follow-up immediately after diagnostic workup” and “no follow-up with pediatric gastroenterologist for 18 months.”
The HRQoL (KIDSCREEN-27) in this study was similar to reference values of European and Swedish children (31,32), and our measured CD-specific HRQoL (CDDUX) agrees with reports from Canada and the Netherlands (7,34). As others (41,42), we found no difference in either generic- or CD-specific HRQoL between children with versus without follow-up of CD.
While most studies have not associated CD with an overall poorer HRQoL, some data suggest a worse HRQoL in children with more pronounced disease symptoms (5–12,28,43). A formal analysis of the association between symptom score and HRQoL was not included in this study. Yet, it is conc
Comments (0)