
Remember me



Short bowel syndrome-associated intestinal failure (SBS-IF) is characterized by impaired gut function leading to malabsorption of macronutrients, fluids, and electrolytes required to maintain growth and development (1). Most patients with SBS-IF experience chronic and debilitating diarrhea, which may be due to accelerated intestinal transit, increased gastrointestinal secretions, small bowel bacterial overgrowth, and malabsorption of carbohydrates, fats, and bile salts (2). Management of SBS-IF includes administration of parenteral nutrition and/or intravenous fluid (PN/IV) that is lifesaving but does not directly address the underlying intestinal malabsorption (1,3,4). Teduglutide, a recombinant human glucagon-like peptide-2 analog (GLP-2), has previously been shown to enhance the structural and functional integrity of the remaining intestine in patients with SBS-IF (5–10). Two phase 3, open-label studies observed reductions in PN/IV and increases in enteral nutrition volume in pediatric patients receiving 0.025 or 0.05 mg/kg teduglutide once daily (11,12).
Diarrhea in children with SBS-IF can lead to malnutrition, dehydration, electrolyte abnormalities, and weight loss, which can greatly impair quality of life, thus increasing the need for PN/IV. Long-term dependence on PN/IV is also associated with potentially life-threatening complications, including hepatic cirrhosis, bloodstream infection, and vascular thrombosis (1,13,14). Clinicians often consider improvements in stool consistency a critical consideration in deciding whether to advance enteral nutrition and wean PN/IV (15).
Following extensive intestinal resection, the remnant bowel undergoes intestinal adaptation, which is a natural process whereby structural and functional changes occur to improve nutrient and fluid absorption via intestinotrophic factors such as GLP-2 (16). GLP-2 inhibits gastric acid secretion and motility, increases intestinal blood flow and barrier function, and enhances nutrient absorption, and therefore is a key promoter of intestinal adaptation (10,17,18). This post-hoc analysis evaluated the effects of teduglutide treatment on stool consistency, frequency, and volume along with changes in enteral nutrition and PN/IV intake using data from previous pediatric SBS-IF clinical trials.
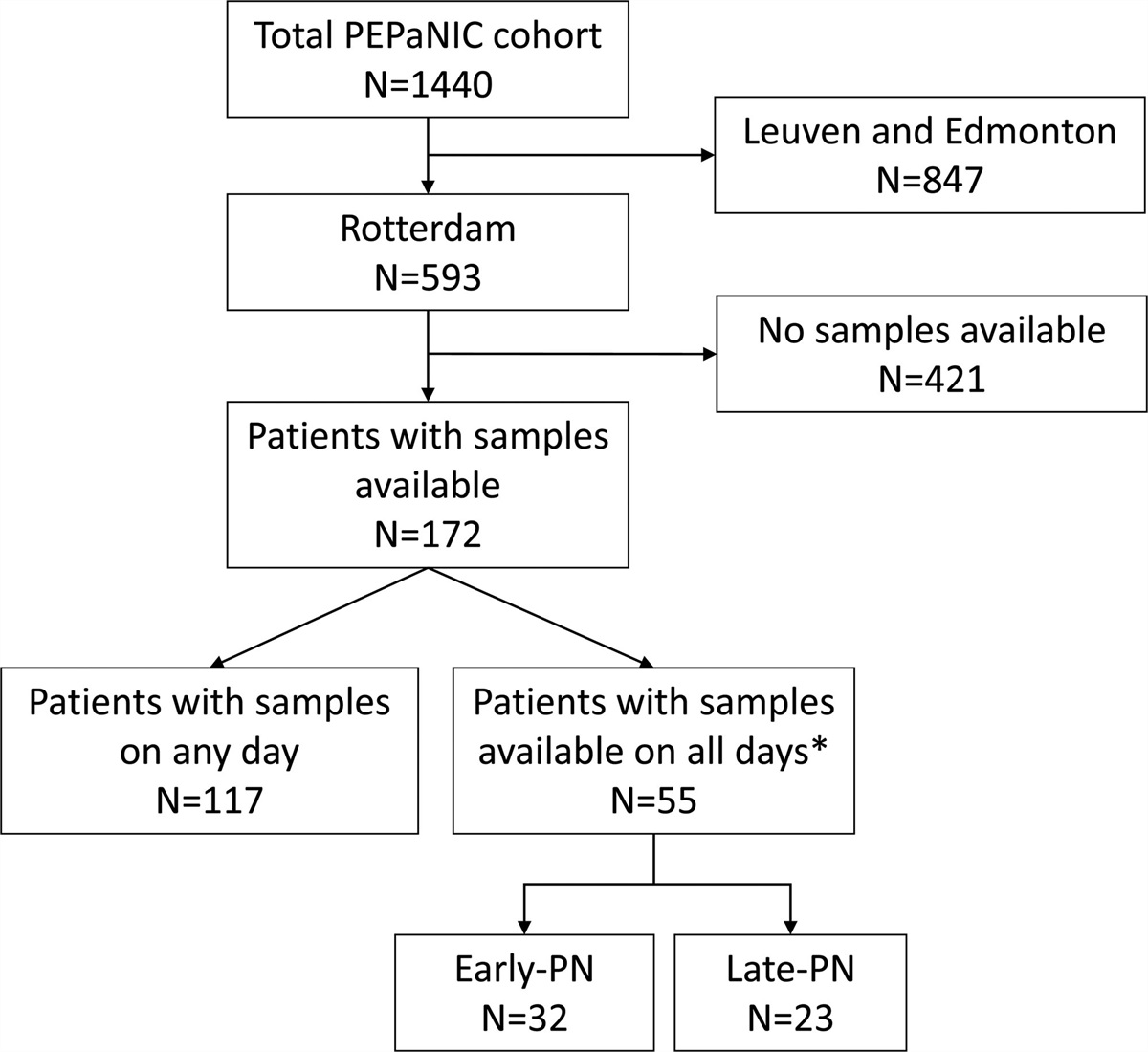
METHODS Study DesignData from 2 phase 3, multicenter, open-label, pediatric SBS-IF clinical trials of teduglutide (NCT01952080 and NCT02682381) were extracted and pooled where possible; data for some parameters were collected in only 1 study. The study period was from November 2013 to January 2015 for NCT01952080, and June 2016 to August 2017 for NCT02682381. Detailed methods for the trials have been published previously (11,12), and patient enrollment from each trial is summarized in Figure 1, Supplemental Digital Content 1, https://links.lww.com/MPG/D273. The “total teduglutide” group includes the number of patients who received subcutaneous teduglutide 0.0125, 0.025, or 0.05 mg/kg/day, where relevant data were collected in both studies. Both trials included a 4-week follow-up period at the end of treatment, during which no teduglutide was received, taking the trials to 16 and 28 weeks, respectively.
Both studies were conducted in compliance with International Council for Harmonization Good Clinical Practice guidelines and the World Medical Association Declaration of Helsinki and its amendments. Local institutional review boards or medical ethics committees approved all protocols, and all parents/legal guardians of study patients provided informed consent.
Assessments and OutcomesThe primary objective of this post-hoc analysis was to evaluate the change in stool characteristics from baseline to weeks 12 and 24, in the context of increasing enteral nutrition following teduglutide treatment. Stool characteristics included consistency [Bristol Stool Form Scale (BSFS) score: an ordinal 7-point scale of stool types ranging from the hardest (type 1) to the softest (type 7)] (19), stool frequency (number of diaper changes per day), and volume (ostomy output, average stool weight, or mixed diaper weight per day). The secondary objective was to assess the change in stool characteristics in relation to potential confounding variables (enteral nutrition intake, PN/IV intake, and urine output) from baseline to weeks 12 and 24. Documentation of enteral intake was limited to specialized enteral formula. Changes from baseline in enteral nutrition and PN/IV were based on patient diary data.
An exploratory objective of this study was to assess the association between disease and patient-level characteristics [eg, underlying short bowel syndrome (SBS) diagnosis, age at SBS onset, residual small bowel length, age at study entry, historical and/or concomitant medication use, enteral nutrition intake, PN/IV intake, urine output) and changes in stool consistency (as measured by the BSFS score) during the study period. Safety assessments included gastrointestinal adverse event (AE) reporting.
Statistical AnalysisDescriptive statistics were used to summarize the baseline and demographic characteristics, and the BSFS summary scores. Efficacy analyses were based on observed cases without inferences for missing data. Patient-level changes between baseline and at weeks 12 and 24 for continuous measures (eg, BSFS score, PN/IV volume, enteral nutrition volume, daily stool frequency) were analyzed using paired t tests. Associations between potential confounding variables and changes in stool consistency were evaluated using analysis of covariance. All analyses were conducted with SAS version 9.4 (SAS Institute, Cary, NC).
RESULTS Baseline Demographics and Disease CharacteristicsA total of 101 patients were included in this pooled analysis: 8, 38, and 41 patients were treated with teduglutide 0.0125, 0.025, and 0.05 mg/kg/day respectively, and 14 patients were in the standard of care (SoC) group. Across all groups, the ages ranged between 1 and 17 years; the proportions of patients with stomas were 12.5%–21.4%; and the proportions of male patients were 64.3%–75.0%. See Table 1 for complete patient demographics and baseline characteristics.
TABLE 1. - Baseline demographics and disease characteristics Parameter Teduglutide SoC (n = 14) 0.0125 mg/kg/day (n = 8) 0.025 mg/kg/day (n = 38) 0.05 mg/kg/day (n = 41) Total (n = 87) Age, y, mean (SD) 5.1 (4.6) 5.9 (3.6) 5.6 (3.6) 5.7 (3.6) 4.4 (4.1) Sex, n (%) Female 2 (25.0) 11 (28.9) 14 (34.1) 27 (31.0) 5 (35.7) Race, n (%) White 6 (75.0) 27 (71.1) 34 (82.9) 67 (77.0) 5 (35.7) Black or African American 2 (25.0) 4 (10.5) 4 (9.8) 10 (11.5) 2 (14.3) Asian 0 (0.0) 1 (2.6) 2 (4.9) 3 (3.4) 2 (14.3) Other 0 (0.0) 6 (15.8) 1 (2.4) 7 (8.0) 5 (35.7) Ethnicity, n (%) Hispanic or Latino 1 (12.5) 11 (28.9) 8 (19.5) 20 (23.0) 4 (28.6) Height z score, mean (SD) 0.3 (0.9) −0.2 (1.35) −0.4 (1.45) −0.3 (1.37) 0.5 (1.7) Weight z score, mean (SD) −0.5 (1.7) −0.2 (1.0) −0.3 (1.0) −0.3 (1.0) 0.2 (1.0) BMI z score, mean (SD) −0.7 (0.7) 0.0 (1.1) −0.1 (1.1) −0.1 (1.1) −0.1 (0.8) SBS history, n (%) Gastroschisis 2 (25.0) 13 (34.2) 17 (41.5) 32 (36.8) 2 (14.3) Intestinal atresia 1 (12.5) 6 (15.8) 3 (7.3) 10 (11.5) 1 (7.1) Long-segment Hirschsprung disease 0 (0.0) 1 (2.6) 1 (2.4) 2 (2.3) 2 (14.3) Midgut volvulus 2 (25.0) 14 (36.8) 13 (31.7) 29 (33.3) 5 (35.7) Necrotizing enterocolitis 1 (12.5) 7 (18.4) 6 (14.6) 14 (16.1) 4 (28.6) Other 2 (25.0) 0 (0.0) 2 (4.9) 4 (4.6) 0 (0.0) Stoma present, n (%)* 1 (12.5) 6 (15.8) 6 (14.6) 13 (14.9) 3 (21.4) Colostomy 0 (0.0) 2 (33.3) 0 (0.0) 2 (15.4) 0 (0.0) Ileostomy 1 (100.0) 1 (16.7) 2 (33.3) 4 (30.8) 1 (33.3) Jejunostomy 0 (0.0) 3 (50.0) 4 (66.7) 7 (53.8) 2 (66.7) Colon present, n (%) 7 (87.5) 36 (94.7) 39 (95.1) 82 (94.3) 11 (78.6) Colon-in-continuity, n (%)† 7 (100.0) 34 (94.4) 36 (92.3) 77 (93.9) 11 (100.0) Estimated remnant small intestine length, cm n 7 33 37 77 14 Mean (SD) 28.1 (25.9) 49.3 (40.1) 41.8 (26.5) 43.8 (33.1) 42.5 (28.5) Median (range) 15.0 (2.0–75.0) 35.0 (4.0–147.0) 40.0 (0.0–120.0) 35.0 (0.0–147.0) 42.0 (5.0–97.5) Ileocecal value present, n (%)‡ 2 (100.0) 7 (70.0) 11 (84.6) 20 (80.0) 4 (100.0)*Percentages are based on patients with stoma in each treatment arm.
†Percentages are based on patients with remaining colon in each treatment arm.
‡Percentages are based on patients with distal/terminal ileum in each treatment arm.
BMI = body mass index; SBS = short bowel syndrome; SD = standard deviation; SoC = standard of care.
At baseline, the mean (standard error; SE) BSFS scores were 6.6 (0.1) and 6.9 (0.1) in the total teduglutide and SoC groups, respectively; the PN/IV volume was 62.4 (3.1) mL/kg/day and 79.6 (6.9) mL/kg/day; and the enteral nutrition volume was 28.1 (3.2) mL/kg/day and 25.5 (8.3) mL/kg/day, respectively (Tables 1–3, Supplemental Digital Content 2–4, https://links.lww.com/MPG/D273).
In the total teduglutide group, at weeks 12 and 24, the absolute mean (SE) BSFS score was 4.8 (0.3) and 4.4 (0.3) respectively, PN/IV volume was 45.6 mL/kg/day (3.1) and 40.9 mL/kg/day (4.1) respectively, and enteral nutrition volume was 38.9 mL/kg/day (4.0) and 35.0 mL/kg/day (5.1), respectively (Tables 1–3, Supplemental Digital Content 2–4, https://links.lww.com/MPG/D273). Furthermore, there were significant changes from baseline to weeks 12 and 24 in mean (SE) BSFS score [−1.8 (0.26; P < 0.0001) and −2.2 (0.27; P < 0.0001), respectively], PN/IV volume [−16.9 (1.7; P < 0.0001) and −20.1 (2.3; P < 0.0001) mL/kg/day, respectively), and enteral nutrition volume [9.2 (1.7; P < 0.0001) and 9.6 (2.3; P = 0.0002) mL/kg/day, respectively]. Between weeks 12 and 24, significant changes were also observed in mean (SE) enteral nutrition volume [3.3 (1.3; P = 0.0133) mL/kg/day]. Among patients receiving SoC, there were no changes in BSFS score and enteral nutrition volume at weeks 12 and 24; PN/IV volume change was −6.9 (1.5; P = 0.0041) at 24 weeks, while no significant change observed at 12 weeks.
The proportion of patients with a BSFS score of ≤ 4 increased from baseline as early as week 4; nearly half of patients receiving teduglutide 0.025 or 0.05 mg/kg/day achieved a BSFS score of ≤ 4 by week 4 through to week 28 (end of study) (Fig. 1). Furthermore, the median BSFS score generally improved from baseline through week 28 in patients receiving teduglutide 0.025 or 0.05 mg/kg/day. In the total teduglutide group (which includes patients receiving teduglutide 0.025 or 0.05 mg/kg/day), the median BSFS score at baseline was 7.0. Reductions in the median BSFS score were observed as early as week 4 (4.8), and further reduced by week 8 (3.5). While the median BSFS score increased at weeks 12 and 16 (5.5 and 6.0, respectively), this was reduced to 3.5 by week 20 and maintained until week 28. Over 50% of patients in the total teduglutide group maintained a BSFS score of ≤ 4 from week 4 through week 28, except for weeks 12 and 16 where < 50% of patients had a BSFS score of ≤ 4 (data not shown).
 FIGURE 1.:
FIGURE 1.: Proportion of patients with a BSFS score of ≤ 4 through week 28. Data were from NCT02682381. The proportion of patients with BSFS ≤ 4 was calculated within every 4-week window. Within each window, patients with at least 1 visit were counted once in the denominator and those with at least 1 BSFS score of ≤ 4 were counted once in the numerator in order to calculate the proportion of patients with a BSFS score of ≤ 4. BSFS = Bristol Stool Form Scale; EoS = end of study; EoT = end of treatment.
Between baseline and week 12, daily stool frequency reduced by 0.8 (0.3) per day in the total teduglutide group (P = 0.0133), but there were no significant changes between baseline and week 24 (Table 4, Supplemental Digital Content 5, https://links.lww.com/MPG/D273). There were no significant changes from baseline observed in diaper change frequency, ileostomy output in average stool, or mixed diaper weight in any of the groups at weeks 12 and 24.
Impact of Disease and Patient Characteristics on Stool ConsistencyAll variables pertaining to disease and patient characteristics had no significant effects on stool consistency as measured by BSFS at weeks 12 or 24 (Table 5, Supplemental Digital Content 6, https://links.lww.com/MPG/D273).
Anti-Diarrheal MedicationsMinimal changes in the mean number of anti-diarrheal doses per day at week 12 or week 24 were observed (Table 6, Supplemental Digital Content 7, https://links.lww.com/MPG/D273). At baseline, the mean [standard deviation (SD)] number of anti-diarrheal doses per day was 3.2 (1.7) in the total teduglutide group and 2.7 (0.6) in the SoC group. At weeks 12 and 24, the mean (SD) number of anti-diarrheal doses per day was 3.1 (1.8) and 2.7 (1.1) in the total teduglutide group, respectively, and 2.7 (0.6) and 3.0 (0.0) in the SoC group, respectively.
SafetyOverall, 86 (98.9%) patients in the total teduglutide group and 14 (100%) patients in the SoC group experienced at least 1 AE, with the majority classed as mild in severity; there were no AEs reported that led to study discontinuation or death. The most common gastrointestinal AEs reported in the total teduglutide group were vomiting, abdominal pain, diarrhea, and nausea (data not shown).
DISCUSSIONThis post-hoc analysis of 2 phase 3 trials provides the clinical trial data on stool characteristics in children with SBS-IF treated with teduglutide. Overall, pediatric patients with SBS-IF receiving teduglutide at a dose of 0.025 or 0.05 mg/kg/day showed significant improvements in stool consistency at week 12 and week 24, despite concurrent increases in enteral formula intake and without a worsening safety profile. Furthermore, the effects of teduglutide treatment in improving stool consistency (as measured by the BSFS score) were observed by week 4, and generally maintained through the end of study.
The present study corroborates previously pediatric studies on the effects of teduglutide on stool consistency. In one study of infants (n = 6) with SBS-IF, a numerical improvement in stool frequency and volume of stoma output was observed after 6 weeks of treatment (20); small improvements in stool frequency were also observed in a separate pediatric trial (n = 7) following 6 weeks of teduglutide treatment (21). The time of response to teduglutide treatment is highly variable due to the heterogeneity of the SBS population; however, this study suggests that teduglutide may provide additional benefit in managing SBS-associated diarrhea in children with SBS-IF in addition to its indication for reducing PN/IV dependence after only 4 weeks of treatment.
The results of this analysis in pediatric patients with SBS-IF are similar to those reported in adult patients (22,23). In a real-world study of 13 adult patients with SBS-IF, teduglutide treatment led to a reduction in stool frequency and improvements in stool consistency despite an increase in meal frequencies and sizes (23). In another real-world study of 14 adult patients with SBS-IF, there was a significant reduction in PN/IV after 24 and 48 weeks of teduglutide treatment; early clinical markers of response included sensation of thirst and stool consistency and frequency (22). Comparable to what is reported in the present study, significant changes in stool frequency and consistency were observed at 12 weeks of treatment, with no further significant changes observed after 12 weeks. Furthermore, teduglutide appeared to have greater impact on stool frequency than on stoma output, emphasizing the importance of the colon in intestinal water conservation (22). Of note, most patients in the present study had a colon-in-continuity, which may explain how improvements in stool consistency were observed as early as week 4.
In this study, the patients’ remnant small intestinal length, a prognostic factor previously associated with spontaneous intestinal adaptation (24), did not have a significant impact on patient stool consistency. Improvement in stool consistency is especially important for patients with SBS-IF, as they experience chronic, lifestyle-altering symptoms of malabsorption that can lead to a significant reduction in their quality of life (25–27). As an intestinotrophic growth factor that binds GLP-2 receptors in the gastrointestinal tract, a GLP-2 receptor agonist such as teduglutide can theoretically address pathophysiologic factors in SBS-associated diarrhea by slowing gastric emptying, reducing gastric secretions, enhancing mucosal barrier function, increasing intestinal blood flow, and stimulating growth of the gastrointestinal epithelium, including increasing crypt depth and villus height (10,17). Other factors, such as microbiota dysbiosis and bile acid malabsorption, are also likely to play an important role. Further studies may help better characterize the full spectrum of SBS-associated diarrhea symptoms, such as tenesmus, nocturnal defecation, frequency, fecal incontinence, and abdominal cramping.
In this study, children with SBS-IF had stools that were entirely liquid and watery with no solid pieces at baseline. From 4 weeks of teduglutide treatment until the end of study, half of the patients had formed stools (defined as a BSFS score of ≤4) with few exceptions. As patients with SBS-IF often experience multiple concurrent issues that could lead to worsening diarrhea, it is not surprising that some patients would have recurrence of unformed stool. During the clinical trials, investigators were given guidelines for nutrition support management and details of the algorithms for weaning off PN/IV based upon urine and stool output. However, management in individual patients also typically required subjective clinical judgments informed by laboratory assessment of hydration and electrolyte balance.
There were no significant improvements in other stool characteristics, such as stool frequency (at week 24), diaper change frequency or diaper weight, and ostomy output. It is unclear whether findings are related to GLP-2 effects on nutrient absorption or gastrointestinal motility. However, it is worth noting that measuring fluid balance in pediatric patients with SBS-IF poses unique methodologic challenges where incontinence is common. Urine output can be a reliable marker of parameters such as drug efficacy, tolerance of PN/IV, and enteral advancement in adult patients with SBS-IF who are able to maintain their continence (8). However, variations in caregiver diaper-changing frequency, stool contamination that can make estimation of urine output difficult, urine leakage, and evaporative loss of urine can lead to inaccuracies when measuring urine output in pediatric patients with SBS-IF wearing diapers.
The study had some limitations. The teduglutide group was exposed to teduglutide treatment and advancing enteral feeds simultaneously. While antidiarrheal agents use did not change over 24 weeks, future studies should explore how antidiarrheal agents use might change during long-term teduglutide treatment. The most significant study limitation was the inadequate power to detect differences between treatment and SoC groups, there was a risk of selection and reporting bias, and data availability limited analyses. For example, data regarding formula intake were available only in terms of specialized formula enteral intake, and other ad lib enteral intake could not be analyzed. A major strength of this study was its inclusion of a large number of pediatric patients with an orphan disease using clinical trial data that were pooled from 2 studies (28). Another strength of this study was using the BSFS, a well-accepted tool for describing stool consistency (19).
CONCLUSIONSIn summary, this post-hoc analysis demonstrates pediatric patients with SBS-IF who were treated with teduglutide 0.025 or 0.05 mg/kg/day showed improvements in stool consistency, which were maintained through 24 weeks. These findings may contribute to clinical management of children with SBS-IF by providing concrete targets for enteral nutrition advancement and PN/IV reduction. Teduglutide was well tolerated, and the overall safety profile was consistent with previous reports in adult and pediatric patients with SBS-IF (7,8,11,12). Further research is needed regarding the impact of patient-level factors on stool characteristics when using teduglutide.
AcknowledgmentsThis study was sponsored by Takeda Pharmaceuticals, Inc. Medical writing assistance was provided by Tina Borg, PhD, of Oxford PharmaGenesis, Oxford, UK, and was funded by Takeda Pharmaceuticals, Inc.
REFERENCES 1. Chandra R, Kesavan A. Current treatment paradigms in pediatric short bowel syndrome. Clin J Gastroenterol. 2018;11:103–12. 2. Kumpf VJ. Pharmacologic management of diarrhea in patients with short bowel syndrome. JPEN J Parenter Enteral Nutr. 2014;38:38S–44S. 3. Bruzoni M, Sudan DL, Cusick RA, Thompson JS. Comparison of short bowel syndrome acquired early in life and during adolescence. Transplantation. 2008;86:63–6. 4. Thompson JS. Short bowel syndrome and malabsorption – causes and prevention. Viszeralmedizin. 2014;30:174–8. 5. Jeppesen PB, Sanguinetti EL, Buchman A, et al. Teduglutide (ALX-0600), a dipeptidyl peptidase IV resistant glucagon-like peptide 2 analogue, improves intestinal function in short bowel syndrome patients. Gut. 2005;54:1224–31. 6. Seidner DL, Joly F, Youssef NN. Effect of teduglutide, a glucagon-like peptide 2 analog, on citrulline levels in patients with short bowel syndrome in two phase III randomized trials. Clin Transl Gastroenterol. 2015;6:e93. 7. Jeppesen PB, Gilroy R, Pertkiewicz M, Allard JP, Messing B, O’Keefe SJ. Randomised placebo-controlled trial of teduglutide in reducing parenteral nutrition and/or intravenous fluid requirements in patients with short bowel syndrome. Gut. 2011;60:902–14. 8. Jeppesen PB, Pertkiewicz M, Messing B, et al. Teduglutide reduces need for parenteral support among patients with short bowel syndrome with intestinal failure. Gastroenterology. 2012;143:1473–1481.e3. 9. Tappenden KA, Edelman J, Joelsson B. Teduglutide enhances structural adaptation of the small intestinal mucosa in patients with short bowel syndrome. J Clin Gastroenterol. 2013;47:602–7. 10. Drucker DJ, Yusta B. Physiology and pharmacology of the enteroendocrine hormone glucagon-like peptide-2. Annu Rev Physiol. 2014;76:561–83. 11. Carter BA, Cohran VC, Cole CR, et al. Outcomes from a 12-week, open-label, multicenter clinical trial of teduglutide in pediatric short bowel syndrome. J Pediatr. 2017;181:102–111.e5. 12. Kocoshis SA, Merritt RJ, Hill S, et al. Safety and efficacy of teduglutide in pediatric patients with intestinal failure due to short bowel syndrome: a 24-week, phase III study. JPEN J Parenter Enteral Nutr. 2020;44:621–31. 13. Bielawska B, Allard JP. Parenteral nutrition and intestinal failure. Nutrients. 2017;9:466. 14. Pironi L, Sasdelli AS. Intestinal failure-associated liver disease. Clin Liver Dis. 2019;23:279–91. 15. Rauh J, Almond A, Glock M, Petty JK, Zeller K. Stool Quality for Intestinal Rehabilitation Therapy (SQUIRT) score. J Pediatr Surg. 2023;58:177–8. 16. Tappenden KA. Intestinal adaptation following resection. JPEN J Parenter Enteral Nutr. 2014;38:23S–31S. 17. Jeppesen PB, Hartmann B, Thulesen J, et al. Glucagon-like peptide 2 improves nutrient absorption and nutritional status in short-bowel patients with no colon. Gastroenterology. 2001;120:806–15. 18. Cheeseman CI, Tsang R. The effect of GIP and glucagon-like peptides on intestinal basolateral membrane hexose transport. Am J Physiol. 1996;271:G477–82. 19. Lewis SJ, Heaton KW. Stool form scale as a useful guide to intestinal transit time. Scand J Gastroenterol. 1997;32:920–4. 20. Sigalet DL, Brindle ME, Boctor D, et al. A safety and pharmacokinetic dosing study of glucagon-like peptide 2 in infants with intestinal failure. J Pediatr Surg. 2017;52:749–54. 21. Sigalet DL, Brindle M, Boctor D, et al. Safety and dosing study of glucagon-like peptide 2 in children with intestinal failure. J Parenter Enteral Nutr. 2017;41:844–52. 22. Schoeler M, Klag T, Wendler J, et al. GLP-2 analog teduglutide significantly reduces need for parenteral nutrition and stool frequency in a real-life setting. Therap Adv Gastroenterol. 2018;11:1756284818793343. 23. Harpain F, Schlager L, Hutterer E, et al. Teduglutide in short bowel syndrome patients: a way back to normal life? JPEN J Parenter Enteral Nutr. 2022;46:300–9. 24. Carbonnel F, Cosnes J, Chevret S, et al. The role of anatomic factors in nutritional autonomy after extensive small bowel resection. JPEN J Parenter Enteral Nutr. 1996;20:275–80. 25. Carlsson E, Bosaeus I, Nordgren S. Quality of life and concerns in patients with short bowel syndrome. Clin Nutr. 2003;22:445–52. 26. Carlsson E, Berglund B, Nordgren S. Living with an ostomy and short bowel syndrome: practical aspects and impact on daily life. J Wound Ostomy Continence Nurs. 2001;28:96–105. 27. Winkler MF, Hagan E, Wetle T, Smith C, Maillet JO, Touger-Decker R. An exploration of quality of life and the experience of living with home parenteral nutrition. JPEN J Parenter Enteral Nutr. 2010;34:395–407. 28. Wales PW, de Silva N, Kim J, Lecce L, To T, Moore A. Neonatal short bowel syndrome: population-based estimates of incidence and mortality rates. J Pediatr Surg. 2004;39:690–5.
Comments (0)