
Remember me






Among the 375 participants enrolled in the study, the mean age was 52.0 years (standard deviation 13.3 years) with a range of 19.7–83.5 years. Detailed characteristics of participants are presented in Table 1. The median duration of HIV infection was 17.0 years with interquartile range 7.0–24.0 years. The overall proportion of participants with well-controlled HIV infection (defined as CD4 ≥ 350 cells/mm3, suppressed HIV viral load), and low number of comorbidities (one or fewer) was 52%. One-third of participants (28.1%) had two or more comorbidities. Most participants (69.1%) had achieved more than a secondary school education (secondary school education comprises schooling up to age 17–18 in Canada). A total of 49 participants had documented COVID-19 infection before study enrolment based on either self-report (n = 25, 51%) or laboratory testing (n = 24, 49%). Eighty-eight participants contracted COVID-19 infection during the study period, up until April 2022, based on either of self-report (n = 54, 61%) and laboratory testing (n = 34, 39%). Of note, the vaccine immunogenicity study is still ongoing so the total number of COVID-19 infections during the total study period is currently unknown. Overall, preventative behaviours were frequently practiced in the cohort, with 87% masking in public, 79% distancing, 70% avoiding large gatherings, and 65% limiting contact with vulnerable persons.
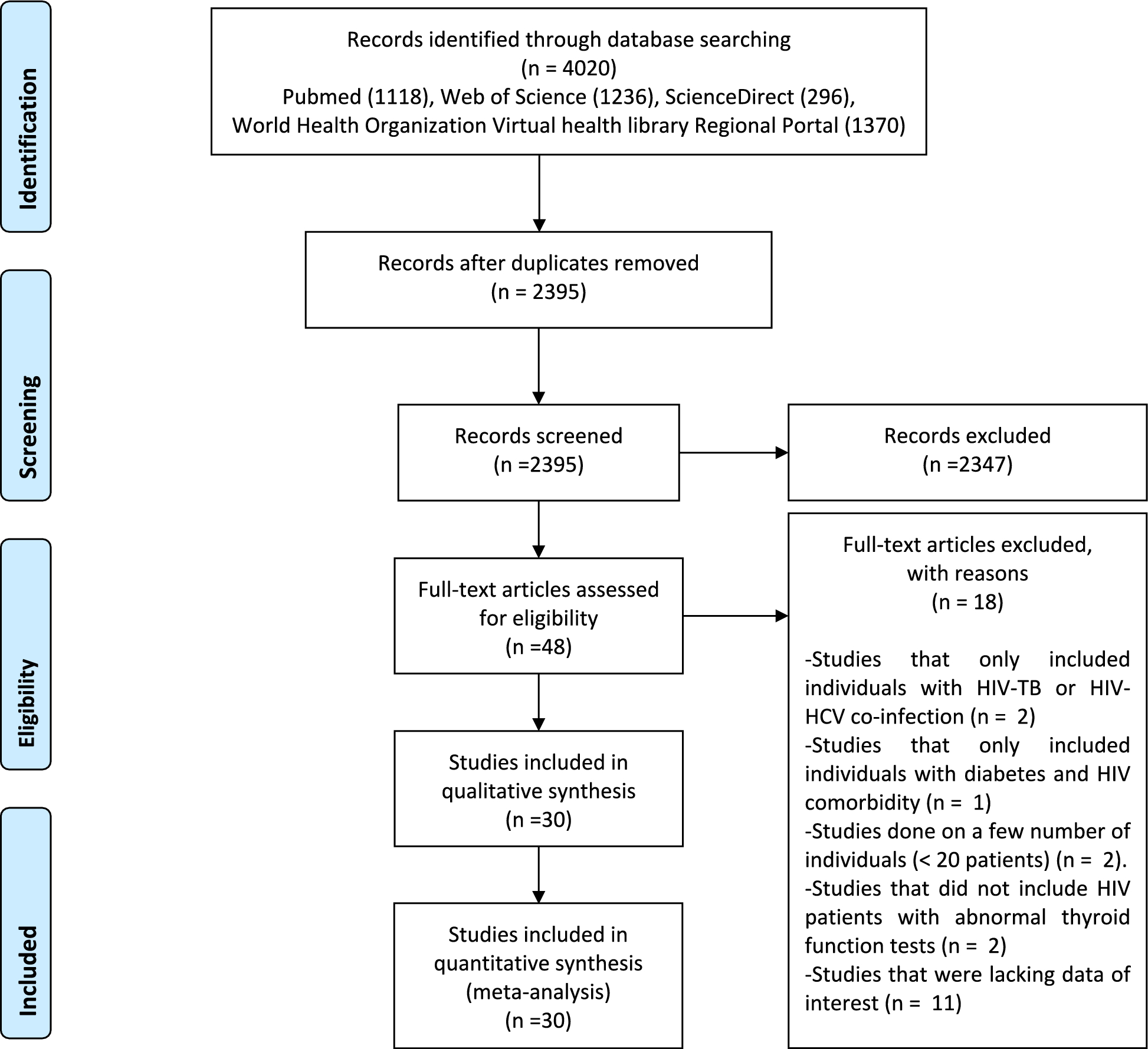
Does previous known COVID-19 infection influence preventative behaviours?To address this question, we excluded individuals with positive serum COVID-19 antibody testing (presumed prior infection) but no knowledge of prior infection (n = 24). A detailed explanation of the participant subsets used in each of the four questions is found in Fig. 1. Participants reporting prior known COVID-19 infection (based on self-report) (n = 25) were more likely to identify as non-white (p < 0.001), less likely to have stable HIV infection (32.0% vs 53.5%, p = 0.039), have more household members (p < 0.001), fewer household bedrooms and bathrooms per person (p = 0.021 and p = 0.006, respectively), and were more likely to be employed in health care (p < 0.001) than those not reporting prior infection. There were no significant differences in the other demographic factors between the prior known infection and non-infected groups. In response to the preventative behaviours survey, participants with prior known COVID-19 were more likely to self-quarantine when thought to have been exposed to COVID-19 but were not symptomatic (p < 0.001) and self-isolate when thought to been infected with COVID-19 (p = 0.021). These differences remained statistically significant after adjusting for age, sex and the aforementioned patient characteristics that were different between groups (aOR = 6.72 [95% CI: 1.98, 22.84], p = 0.002 and 3.50 [95% CI: 1.09, 11.21], p = 0.035 respectively). These were the only significant differences in preventative behaviours between groups.
Fig. 1
Flowchart demonstrating subsets of the cohort used to answer four questions related to participant demographics and COVID-19 preventative behaviours
Is participant multimorbidity associated with preventative behaviour practices?Participants in the multimorbidity group were more likely to be older (mean age 59.2 years vs 49.0 years, p < 0.001), live in a household with fewer members (p = 0.020), have more bedrooms and bathrooms in the household per person (p = 0.019 and p = 0.008, respectively), usually get an influenza immunization (p = 0.045), and less likely to be performing paid or unpaid work in close physical proximity to others (p = 0.035). They were more likely to be vaccinated with four doses against COVID-19 by September 2022 (33.7% vs 16.7%, p = 0.001). In response to the preventative behaviours survey, participants in the multimorbidity group were more likely to be practicing physical distancing (85.7% vs 75.5%, p = 0.044). This difference, however, was no longer statistically significant after adjusting for participant characteristics (age, sex, race, number of household members, number of bedrooms and bathrooms in the household per person, uptake of influenza immunization and performing paid or unpaid work in close physical proximity to others) (aOR = 1.74 [95% CI: 0.84, 3.58], p = 0.140), and no other significant differences in preventative behaviours between groups were noted.
Are preventative behaviour practices, living in a crowded space, and working in close proximity to others associated with COVID-19 infection?The participants in the COVID-19 infection group were more likely to have fewer bedrooms per person (mean 1.0 vs 1.3, p = 0.006). There were no identified differences in the proportion of participants performing paid or unpaid work in close physical proximity to others between those with and without COVID-19 infection (28.2% vs 32.9%, p = 0.429). There were no identified differences in preventative behavior practices between those with and without baseline COVID-19 infection.
Are preventative behaviour practices and/or uptake of COVID-19 vaccination associated with developing symptomatic COVID-19 infection during the highly contagious Omicron wave?In Canada, the Omicron wave began in late November 2021 [9]. Participants in the Omicron infection group were more likely to have been tested for COVID-19 at some point before study enrolment (p = 0.015). There was no statistical difference in Omicron infection rate by COVID-19 vaccination status at the start of the Omicron wave (26.9% versus 16.0% for those who received 3 vaccine doses versus less than 3 doses, p = 0.065). The finding was the same after adjusting for age, sex, race, multimorbidity, number of household members, number of bedrooms and bathrooms in the household per person and performing paid/unpaid work in close physical proximity to others (aOR = 1.84 [95% CI: 0.80, 4.22], p = 0.150). There were no significant differences in preventative behaviours between those sustaining COVID-19 infection during the Omicron wave and those not infected during this time period.
Comments (0)