
Remember me


Primary hepatic angiosarcoma is a noncirrhotic malignancy of the liver of endothelial cell origin. It accounts for 2% of all liver tumors and is the sixth most common primary location of angiosarcoma.1 Historically, it has been associated with toxins such as thorotrast, vinyl chloride, anabolic steroids, and exogenous steroids, but most cases do not have a clear causative factor.2 Hepatic angiosarcoma is extremely difficult to diagnose because many patients are asymptomatic, with only 9% of patients presenting with symptoms secondary to metastasis.3 The typical symptoms include abdominal pain, fatigue, anorexia, and weight loss. Hemoperitoneum from spontaneous tumor rupture occurs in 17% to 27% of cases, which makes obtaining tissue samples for histopathologic diagnosis highly challenging.4,5 Anemia and thrombocytopenia are the most common laboratory abnormalities and are thought to occur due to the consumption of clotting factors. Patients with liver angiosarcoma exhibit coagulation system dysregulation. As a result, they can present with Kasabach-Merritt syndrome, which is characterized by thrombocytopenia and hyperconsumption of coagulation factors within a vascular tumor.6,7 Distant metastases are present in >60% of cases. The lung and hilar lymph nodes are the most common sites of metastasis, followed by the spleen and bones.5,8 The median survival is dismal at 6 months, with only 3% of patients living for more than 2 years even after aggressive treatment.9
Liver angiosarcoma is challenging to manage because of its rapid progression, propensity to metastasize early in its clinical course, and high recurrence rates. Moreover, there is a lack of standardized treatment options for targeting this highly aggressive disease. This study details the clinical characteristics and treatment outcomes of patients with primary liver angiosarcoma treated at an academic sarcoma center, as well as our perspectives on overall disease management.
METHODS Data CollectionAll patients with primary liver angiosarcoma treated at our institution between 2000 and 2022 were screened for this study. Stanford sarcoma pathologists reviewed the samples and determined the diagnoses. Data was collected from the EPIC electronic medical records and included patient demographics, tumor characteristics based on pathology reports, Next-Generation Sequencing (NGS) when available from tumor samples, treatment modalities, and patient outcomes. The treatment modalities included surgery, radiotherapy, embolization, chemotherapy, and immunotherapy. Survival status was determined through a chart review of Stanford EPIC records. The database lock date was February 12, 2023.
Tumor ClassificationThe diagnosis of angiosarcoma was confirmed by a board-certified surgical pathologist specializing in sarcoma pathology (G.W.C.). Tumor classification was performed using the histologic criteria of the WHO classification of soft tissue and bone tumors (fifth edition).10 Primary liver angiosarcoma is histologically defined as a malignant vascular neoplasm that exhibits endothelial-type differentiation. The primary diagnostic morphologic feature was vasoformation by neoplastic cells, while the most important immunohistochemical feature was CD31 and ERG expression.
Statistical AnalysisPython 3.0 was utilized to perform statistical analysis. The Kaplan-Meier method and Lifeline packages were used to create survival curves. There was insufficient data to generate curves comparing survival outcomes based on treatment modality. A P value threshold of 0.05 was used to determine statistical significance.
RESULTS Patient CharacteristicsFifty consecutive patients were identified using the institutional diagnostic archive database queried for the terms “liver” and “angiosarcoma.” Eligibility criteria included patients with pathology reports indicating a diagnosis of primary liver angiosarcoma as well as those receiving diagnosis and/or treatment through our Sarcoma Center. Twenty-three out of 50 patients were eligible for inclusion in the study. Twenty-three patients had pathology reports, while 14 of the 23 patients also had management data. Nine of the 23 patients were also included for purposes of demographic information. Four of the 14 patients were transitioned to hospice care at the time of diagnosis. The 27 patients who were excluded had secondary liver involvement by angiosarcoma and/or had incomplete pathology reports. Overall patient characteristics are summarized in Table 1. There were slightly more females (12) than males (11), with a median age at diagnosis of 65 years (range of 39 to 89 years).
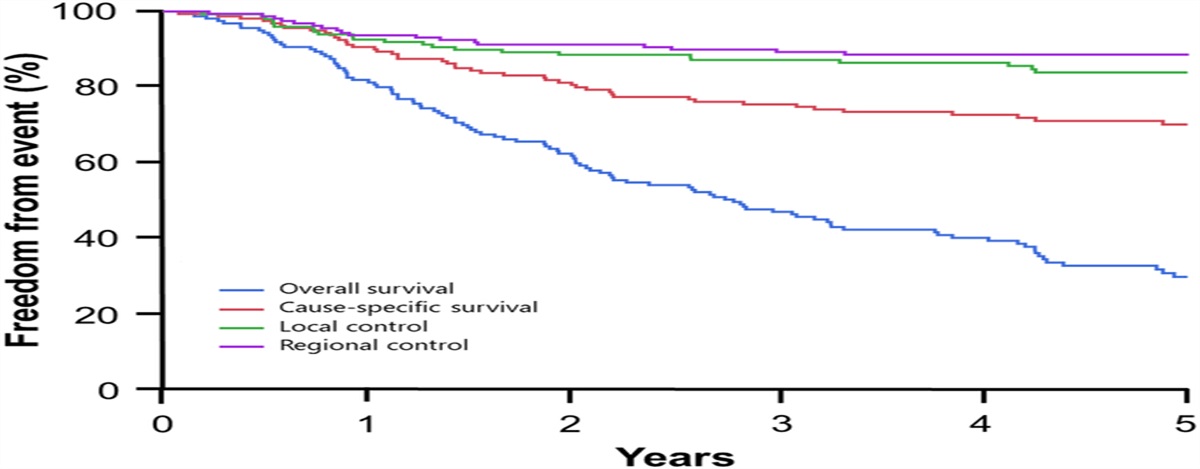
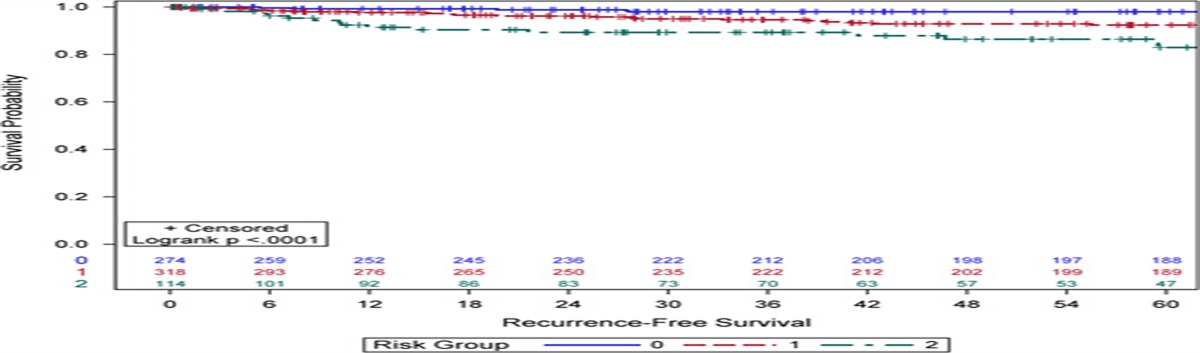
TABLE 1 - Summary of Patient Characteristics Characteristics Frequency % Total (overall) 23 100 Sex Male 11 48 Female 12 52 Age group (y) <40 1 4 40–49 5 22 50–59 2 9 60–69 6 26 70–79 7 30 80–89 2 9 Race White 14 61 Asian 3 13 Hispanic 1 4 Other 5 22 Location Bilobar 13 57 Right Lobe 5 22 Left Lobe 1 4 Unknown 4 17The median overall survival (OS) for patients was 6 months, with a range of 0.07 to 222.6 months. Two-year and 5-year survival rates were both 38.6% (Fig. 1). Overall treatment modalities are summarized in Table 2. Most of the patients received systemic chemotherapy (71%, 10 of 14). Four of the 14 (29%) patients received immunotherapy. Two of the 14 (14%) patients had surgery or radioembolization, while only 1 patient was treated with radiotherapy. One patient underwent Yttrium 90 radioembolization as a fourth-line treatment and exhibited 4 months of progression-free survival (PFS) with an OS of 15 months. Another patient who underwent Yttrium 90 radioembolization as second-line treatment in conjunction with ipilimumab/nivolumab had an OS of 6 months.
 FIGURE 1:
FIGURE 1: Kaplan-Meier Curve Showing Overall Survival (OS) for Patients.
TABLE 2 - Summary of Treatment Data Treatment (n=14) n (%) PFS (mo) Treatment type Surgery 2 (14) — Radiation 1 (7) — Radioembolization 2 (14) — Chemotherapy 10 (71) — Immunotherapy 4 (29) — Regimen Doxorubicin 1 (7) 2 Sunitinib 1 (7) — Paclitaxel 2 (14) 1.5 XL-647 1 (7) 186 Gemcitabine/Paclitaxel 1 (7) — Doxorubicin/HES Anti-TRAIL Ab 1 (7) 7 Gemcitabine/Docetaxel 4 (29) 10 Ipilimumab/Nivolumab 1 (7) 17.6 Pembroluzimab (adjuvant)/Radiation 1 (7) 9 Ifosfamide/Etoposide/Bevacizumab 1 (7) 2 Nab-Paclitaxel/Gemcitabine/Pembroluzimab 1 (7) 2 Doxorubicin/Ifosfamide/Mesna 1 (7) 7 Gemcitabine/Docetaxel (adjuvant)/Surgery 1 (7) 16 Ipilimumab/Nivolumab/Radioembolization 1 (7) 2.5Three patients in our cohort responded particularly well to treatment. Next-generation sequencing (NGS) was available for 2 patients. One patient’s tumor showed alterations in KDR, TP53, and PTPRB. This patient had an OS of 15 months. He was treated with 4 lines of treatment: doxorubicin/ifosfamide/mesna, nab-paclitaxel/gemcitabine/pembroluzimab, ifosfamide/etoposide/bevacizumab, and radioembolization. The other patient’s NGS (Case 3 below) showed alterations in NF1, ATRX, DNMT3A, NOTCH1, and TP53.
Case 1: A 39-year-old woman with a medical history of renal failure, renal transplant, and high-grade transitional cell carcinoma with recurrence s/p bilateral nephroureterectomy. During routine surveillance imaging for her history of transitional cell carcinoma, an MRI of the abdomen and pelvis showed 2 hepatic lesions, 1 of which was a malignant lesion. She underwent laparoscopic resection of the lesion. The patient completed 3 cycles of adjuvant treatment with gemcitabine and docetaxel. Subsequent surveillance imaging showed no new evidence of disease until an MRI of the abdomen and pelvis 9 months later demonstrated a new focus of delayed enhancement in hepatic segment 8. The patient ultimately underwent a right-sided hepatectomy, given this finding. Interestingly, pathology did not indicate any residual hepatic angiosarcoma. She continues to do well with no recurrence at 80 months.
Case 2: A 60-year-old woman with worsening abdominal pain and subsequent computed tomographic images with evidence of multiple lesions in both liver lobes. A biopsy of the liver lesion revealed a well-differentiated angiosarcoma. Despite no interval growth of the liver lesions on CT imaging, the patient received 5 cycles of doxorubicin with a monoclonal antibody against TRAIL-R2 receptor (HGS-ETR2) to minimize the risk of progression. Scans displayed a partial response to treatment, but the patient eventually stopped treatment due to side effects. Although subsequent surveillance scans showed no significant progression of the disease, she was started on tesevatinib (XL-647), a multitargeted tyrosine kinase inhibitor. She exhibited stable disease in response to treatment but ultimately stopped treatment due to side effects. She continues to exhibit stable disease today with a PFS of 186 months.
Case 3: A 84-year-old woman with progressively worsening abdominal pain was found to have multiple septate lesions in the liver and spleen on imaging. An initial biopsy of the right-sided liver lesion showed no evidence of neoplasm. Follow-up MRI and CT of the abdomen/pelvis indicated stable liver and spleen lesions, with new lytic lesions of the spine. Subsequent repeat biopsy of the liver lesion revealed angiosarcoma. She could not tolerate paclitaxel and pazopanib and received 6 cycles of ipilimumab/nivolumab, followed by 9 cycles of maintenance nivolumab. Follow-up scans demonstrated a partial response. Immunotherapy was ultimately stopped due to immune-mediated pneumonitis. Given the progression in size of the splenic lesion on follow-up CT imaging, radiotherapy was administered. The tumors remain stable currently, and the patient exhibits a PFS of 17.6 months.
DISCUSSIONAngiosarcoma is a rare and aggressive malignant tumor that accounts for less than 2% of all sarcomas.11 Moreover, 60% of angiosarcomas originate in the skin, most commonly in the head and neck, but can present in a diverse array of locations such as soft tissues, retroperitoneum, bone, and visceral organs. The pathogenesis of angiosarcomas is unknown, but risk factors include a history of radiation, chronic lymphedema (Stewart-Treves Syndrome), and genetic syndromes such as bilateral retinoblastoma, Recklinghausen neurofibromatosis, and Xeroderma pigmentosa.2 Liver angiosarcoma, in particular, is a malignant mesenchymal tumor of the liver in adults that represents 2% of all primary hepatic malignancies. Although 75% of liver angiosarcomas have no known etiology, environmental carcinogens such as vinyl chloride, thorium dioxide, and arsenic are considered rare risk factors.3,4,12
In our study, there were slightly more females than males diagnosed with primary liver angiosarcoma, with a median age at diagnosis of 65. The age at diagnosis in our study was mostly consistent with the current literature, although there are several retrospective studies that indicate a median age range of 50 to 59. The almost equal distribution of gender among our patients was in contrast to the current literature, typically demonstrating a male-to-female ratio of 2 to 3:1.1,13–15 Most of our patients had bilobar disease, which is consistent with the current literature.16–18 The median OS for our patients was poor at 6 months. It was higher than the median OS of ~2 months described in retrospective studies analyzing treatment outcomes in the National Cancer Database and Surveillance, Epidemiology, and End Results Registry (SEER) database.19,20 However, it was comparable to survival rates reported in other retrospective and meta-analysis studies.16,17,21 Two-year and 5-year OS rates were both 38.6%. Other retrospective studies have demonstrated both higher and lower OS rates.13,16,22
Standardized treatment data for primary hepatic angiosarcoma is limited, given the small number of case reports and case series in the current literature. Surgical resection is the only known curative treatment modality for primary hepatic angiosarcoma.13 In our study, we found that the 2 patients who underwent surgical resection had a higher OS of 24.7 and 100.8 months compared with the median OS of 6 months. Surgery was able to confer long-term survival in one of these patients. This is consistent with the current literature illustrating a significantly higher OS for patients with hepatic liver angiosarcoma who underwent surgery than for those who did not. It is important to note that patients who are surgical candidates have a lower tumor burden than those who are not surgical candidates.13,20,23 A prospective study conducted by Tripke et al reported a median OS of 59 months and a PFS of 11 months for patients who underwent surgical resection with negative margins.23 It is important to note that hepatic resection is only beneficial when the lesion is localized to one lobe of the liver in the setting of no metastatic disease. Therefore, most hepatic angiosarcomas at the time of diagnosis are deemed unresectable.6 Only 14% of the patients in our study underwent surgical resection, which is comparable to other retrospective studies.14,19–21 Surgical resection is most beneficial when the tumor size is less than 10 cm, as the risk of intraoperative complications, such as intraperitoneal hemorrhage, increases with tumor size.20 Hepatic angiosarcoma is also considered an absolute contraindication to liver transplantation, given its poor survival outcomes, high rates of tumor recurrence, and high rates of infection.24
Chemotherapy has not shown a clear survival benefit in this patient population. The most commonly employed chemotherapy regimens in our study included paclitaxel and gemcitabine/docetaxel, which is similar to regimens employed in a retrospective multi-institutional study but in contrast to a meta-analysis that found that alkylating agents and anthracyclines were most commonly used.16,25 Adjuvant treatment with gemcitabine/docetaxel after hepatic resection conferred the second-highest OS in our study of 100.8 months, which may have been due to initial resection. Another patient in our study who received gemcitabine/docetaxel when progressing after hepatic resection displayed a PFS of 19 months and an OS of 24.7 months, which was higher than the median OS of 6 months. Overall, patients in our study who received gemcitabine/docetaxel for unresectable disease responded fairly well, with a median PFS of 10 months. The retrospective study by Mangla and colleagues, which analyzed treatment outcomes for primary hepatic angiosarcoma through the National Cancer database, demonstrated a median OS of 5.1 months for patients who underwent chemotherapy versus 1.2 months for patients who did not. Ultimately, this study, as well as another retrospective multi-institutional study, indicated no long-term benefits from chemotherapy.16,19 A retrospective study demonstrated improvements in the quality of life and duration of survival in patients with vinyl chloride-associated angiosarcoma who received doxorubicin, cyclophosphamide, and methotrexate.26 Doxorubicin, in combination with cyclophosphamide, methotrexate, and thalidomide with adjuvant radiotherapy, has shown efficacy in prolonging OS and PFS in case reports.26,27 No studies have explored the role of immunotherapy in the treatment of liver angiosarcoma. One patient in our study received adjuvant immunotherapy with pembrolizumab in conjunction with radiation and displayed a PFS of 9 months, while another patient received ipilimumab and nivolumab with radioembolization and had an OS of 6 months. The patient from Case 3 in our results section demonstrated a PFS of 17.6 months in response to ipilimumab and nivolumab and is still alive at 25.2 months since diagnosis, which could indicate a potentially promising role of immunotherapy in improving liver angiosarcoma survival outcomes.
Similar to systemic chemotherapy, a clear survival benefit from transcatheter arterial chemoembolization (TACE) and yttrium 90 radioembolization has not been established in the current literature. While no patients underwent TACE in our study, 2 patients underwent radioembolization and had an OS of 6 months and 15 months, respectively. A retrospective study illustrated the benefits of TACE in regard to decreasing tumor size and increasing OS, specifically in patients with a dominant large liver mass.28 Adjuvant TACE after hepatic surgery also demonstrated a recurrence-free survival of 64 months in 1 case, while TACE in the absence of surgery was performed in 2 patients in another study who survived 16 months and 11 months, respectively.14,29 A multicenter retrospective study assessing the response and OS for radioembolization of hepatic sarcomas showed a significant increase in OS and objective response rate with minimal adverse effects.30 An overall summary of treatment modalities and outcomes of primary hepatic angiosarcoma from previous retrospective and prospective studies is presented in Table 3.
TABLE 3 - Summary of Treatment Modalities and Clinical Outcomes of Primary Hepatic Angiosarcoma Based on Previous Retrospective and Prospective Studies References Time period No. patients (n) Treatment modalities Clinical outcomes Dannaher et al26 1974–1976 4 Adriamycin/cytoxan/methotrexate (n=3); adriamycin (n=1) Median OS: 14 mo Kim et al6 1985–2007 5 Docetaxel/cisplatin/flouracil (n=2); docetaxel/cisplatin/flouracil, ifosfamide/doxorubicin through hepatic artery, ifosfamide/doxorubicin (n=1); ifosfamide/doxorubicin, paclitaxel, bevacizumab (n=1); conservative therapy (n=1) Median OS: 2.8 mo Duan et al22 1999–2005 6 Curative hepatic resection (n=4); curative hepatic resection +carboplatin/pirarubicin (n=1); palliative hepatic resection (n=1) Curative resection: 1 y OS: 100%; 3 y OS: 80%; 5 y OS: 40% Wilson et al16 1999–2017 44 Surgical resection (n=10); TACE, radioembolization, or external beam radiation (n=6); systemic treatment (taxol-based regimen, mitomycin/adriamycin/cisplatin, gemcitabine-based regimen, pazopanib, bevacizumab) (n=18); conservative therapy (n=13) 1 y OS: 30%; 3 y OS: 8.1%; 5 y OS: 5.6% Park et al28 2002–2007 6 TACE (n=4); TAE (n=2) Median OS: 3.5 mo Hur et al17 2002–2012 8 Hepatic resection (n=1); TACE (n=1); systemic treatment (doxorubicin/ifosfamide +/- docetaxel or paclitaxel) (n=4); conservative therapy (n=2) Median OS: 7 mo Tripke et al23 2002–2017 9 Surgical resection (n=4); neoadjuvant paclitaxel+surgical resection (n=1); surgical resection+adjuvant doxorubicin/ifosfamide (n=1); surgical resection+paclitaxel (n=1); surgical resection+TACE+ifosfamide/doxorubicin (n=1) Median OS: 7 moLiver angiosarcomas exhibit high genetic heterogeneity, which are characterized by KRAS mutations that predominantly affect codons 12 and 13 in patients exposed to Vinyl Chloride.31 Whole genome sequencing has also characterized genomic alterations in Collagen Type 1 alpha 1 chain (COL1A), Heparan Sulfate Proteoglycan 2 (HSPG2), and BRCA1 and BRCA2 mutations.32 A retrospective study exploring NGS of Chinese hepatic angiosarcoma patients without occupational exposure found that the most commonly altered genes were TP53 and ATRX, while 60% of patients with ATRX inactivation also showed high tumor mutational burden values. Twenty-nine percent of patients also had positive PD-L1 expression.33 There have also been cases describing the fusion of ROS1 with GOPC/FIG as well as BRAF V600E, which raises the possibility of the use of drugs such as crizotinib and vemurafenib, respectively.34,35 Interestingly, a retrospective study analyzing genomic biomarkers with angiosarcomas based on the site of origin found that MYC amplification was not found in any visceral angiosarcomas.36 In our study, NGS was available for 2 patients. These 2 patients exhibited mutations in KDR, TP53, and PTPRB as well as NF1, ATRX, DNMT3A, NOTCH1, and TP53, respectively.
Our study illustrates that primary liver angiosarcomas continue to have poor OS and outcomes. Although this study is one of the larger retrospective studies at an academic institution involving patients with liver angiosarcoma, there were not enough cases to compare survival outcomes between treatment modalities. Given the dearth of retrospective and prospective studies on the treatment outcomes of primary liver angiosarcoma, there is no standardized treatment for this devastating disease. Surgical resection with negative margins has been shown to be the most effective treatment modality in the literature. No clear benefit has been consistently shown with chemoembolization, radioembolization, or chemotherapy. However, there are a small number of cases from retrospective studies, and case reports that have demonstrated improved survival with these modalities. More studies are needed to determine the efficacy of these treatment modalities, which is especially crucial in patients with unresectable diseases. Interestingly, there have been no studies exploring the role of immunotherapy in the treatment of primary liver angiosarcoma. Further research is also needed to elucidate the genetics of this disease and determine if there are targeted treatments, such as immunotherapy, that can improve survival outcomes.
Our study has several limitations. The retrospective nature of this study makes it subject to selection bias and the initiation of particular types of treatment based on disease characteristics and severity. Unfortunately, genomic data was unavailable for most of our patients. In addition, further treatment data were not available for certain patients after pursuing initial care at Stanford, given that they continued care at outside institutions where we did not have access to medical records. Although our study is one of the larger retrospective studies involving patients with liver angiosarcoma, the small sample size still poses a limiting factor.
In conclusion, our findings indicate that primary liver angiosarcoma has poor outcomes despite treatment. Surgical resection has been shown to be the most effective treatment modality in the literature and also increased the OS of patients in our study. However, surgery is often highly difficult to complete as many patients have advanced or unresectable diseases at diagnosis. Overall management of this disease is further challenged by the fact that there is no accepted systemic standardized treatment that has shown benefit. Early diagnosis is key to maximizing the chances of viable surgery. Further research is essential to illuminate the clinical course of this devastating disease and effective treatment options so that overall treatment outcomes can be improved.
REFERENCES 1. Averbukh LD, Mavilia MG, Einstein MM. Hepatic angiosarcoma: a challenging diagnosis. Cureus. 2018. 2. Young RJ, Brown NJ, Reed MW, et al. Angiosarcoma. Lancet Oncol. 2010;11:983–991. 3. Chaudhary P, Bhadana U, Singh RAK, et al. Primary hepatic angiosarcoma. EJSO. 2015;41:1137–1143. 4. Zhu YP, Chen YM, Matro E, et al. Primary hepatic angiosarcoma: A Report of two cases and literature review. WJG. 2015;21:6088–6096. 5. Locker GY, Doroshow JH, Zwelling LA, et al. The clinical features of hepatic angiosarcoma: a report of four cases and a review of the English Literature. Medicine. 1979;58:48–64. 6. Kim HR, Rha SY, Cheon SH, et al. Clinical features and treatment outcomes of advanced stage primary hepatic angiosarcoma. Ann Oncol. 2009;20:780–787. 7. Wadhwa S, Kim TH, Lin L, et al. Hepatic angiosarcoma with clinical and histological features of Kasabach-Merritt Syndrome. WJG. 2017;23:2443. 8. Kumar A, Sharma B, Samant H. Liver Angiosarcoma. Statpearls. 2022. 9. Chien CY, Hwang C, Yeh C, et al. Liver angiosarcoma, a rare liver malignancy, presented with intraabdominal bleeding due to rupture- a Case Report. World J Surg Onc. 2012;10:23. 10. WHO Classification of Tumours Editorial Board. Soft Tissue and Bone Tumours; World health organization classification of tumours. International Agency for Research on Cancer, Lyon, France. 2020:176–177. 11. Cao J, Wang J, He C, et al. Angiosarcoma: A review of diagnosis and current treatment. Am J Cancer Res. 2019;9:2303–2313. 12. Florou V, Wilky BA. Current and future directions for angiosarcoma therapy. Curr Treat Options in Oncol. 2018;19:14. 13. Huang NC, Kuo YC, Chiang JC, et al. Hepatic angiosarcoma may have fair survival nowadays. Medicine. 2015;94:e816. 14. Jiang S, Wu H, Lu M, et al. Surgery and chemotherapy improve the prognosis of primary hepatic angiosarcoma: a retrospective study based on propensity score matched survival analysis. Eur J Surg Oncol. 2021;47:690–698. 15. Jiang L, Xie L, Li G, et al. Clinical characteristics and surgical treatments of primary hepatic angiosarcoma. BMC Gastroenterol. 2021;21:156. 16. Wilson GC, Lluis N, Nalesnik MA, et al. Hepatic angiosarcoma: a multi-institutional, international experience with 44 cases. Ann Surg Oncol. 2019;26:576–582. 17. Hur CJ, Min BR, Lee YJ, et al. Clinical courses of primary hepatic angiosarcoma: retrospective analysis of eight cases. Korean J Gastroenterol. 2015;65:229. 18. Huang NC, Wann SR, Chang HT, et al. Arsenic, Vinyl chloride, viral hepatitis, and hepatic angiosarcoma: a hospital-based study and review of literature in Taiwan. BMC Gastroenterol. 2011;11:142. 19. Mangla A, Cioffi G, Barnholtz-Sloan JS, et al. Treatment Outcomes for primary hepatic angiosarcoma: National Cancer Database Analysis 2004-2014. Curr Oncol. 2022;29:3637–3646. 20. Martínez C, Lai JK, Ramai D, et al. Cancer Registry Study of malignant hepatic vascular tumors: hepatic angiosarcomas and hepatic epithelioid hemangioendotheliomas. Cancer Med. 2021;10:8883–8890. 21. Zheng Y, Zhang X, Zhang J, et al. Primary hepatic angiosarcoma and potential treatment options: hepatic angiosarcoma and treatment options. J Gastroenterol Hepatol. 2014;29:906–911. 22. Duan XF, Li Q. Primary hepatic angiosarcoma: a retrospective analysis of 6 cases: review of six hepatic angiosarcoma cases. J Digest Dis. 2012;13:381–385. 23. Tripke V, Heinrich S, Huber T, et al. Surgical therapy of primary hepatic angiosarcoma. BMC Surg. 2019;19:5. doi:10.1186/s12893-018-0465-5 24. Tran Minh M, Mazzola A, Perdigao F. Primary hepatic angiosarcoma and liver transplantation: radiological, surgical, histological findings and clinical outcome. Clin Res Hepatol Gastroenterol. 2018;42:17–23. 25. Li DB, Si XY, Wan T, et al. A pooled analysis of treatment and prognosis of hepatic angiosarcoma in adults. Hepatobiliary Pancreat Dis Int. 2018;17:198–203. 26. Dannaher CL, Tamburro CH, Yam LT. Chemotherapy of Vinyl Chloride-Associated Hepatic Angiosarcoma. Cancer. 1981;47:466–469. 27. Kayaci S, Yildiz O, Gucer H, et al. Angiosarcoma of the liver with metastasis to the cervical spine cured with the treatment of thalidomide and radiotherapy. Acta Neurochir. 2012;154:369–370. 28. Park YS, Kim JH, Kim KW, et al. Primary hepatic angiosarcoma: imaging findings and palliative treatment with transcatheter arterial chemoembolization or embolization. Clin Radiol. 2009;64:779–785. 29. Ozden I, Bilge O, Erkan M, et al. Five years and 4 months of recurrence-free survival in hepatic angiosarcoma. J Hepatobiliary Pancreat Surg. 2003;10:250–252. 30. Miller MD, Sze DY, Padia SA, et al. Response and Overall Survival for Yttrium-90 Radioembolization of Hepatic Sarcoma: a Multicenter Retrospective Study. J Vasc Interv Radiol. 2018;29:867–873. 31. Weihrauch M, Bader M, Lehnert G, et al. Mutation analysis of K-Ras-2 in liver angiosarcoma and adjacent nonneoplastic liver tissue from patients occupationally exposed to vinyl chloride. Environ Mol Mutagen. 2002;40:36–40. 32. Goerlitz DS, Blancato J, Ramesh A, et al. Somatic mutation signatures in primary liver tumors of workers exposed to ionizing radiation. Sci Rep. 2019;9:18199. 33. Luo R, Zhang L, Jiang Z, et al. Abstract 742: Genomic alteration, tumor mutation burden and PD-L1 status of Chinese hepatic angiosarcoma patients. Cancer Res. 2019;79:742–742. 34. Marks EI, Pamarthy S, Dizon D, et al. ROS1-GOPC/FIG : a novel gene fusion in hepatic angiosarcoma. Oncotarget. 2019;10:245–251. 35. Wilson M, Xu R. Metastatic Hepatic Angiosarcoma and BRAF Inhibitor Therapy. J Clin Epigenet. 2017;3:51. doi:10.21767/2472-1158.100085 36. Espejo-Freire A, Elliott A, Rosenberg A, et al. Genomic landscape of angiosarcoma: a targeted and immunotherapy biomarker analysis. Cancers. 2021;13:4816.
Comments (0)