
Remember me
A term female newborn infant with a birth weight of 3.2 kg and prenatal diagnosis of jejunal atresia was delivered by elective C-section due to previous maternal obstetrical history (Fig. 1). A post-natal abdominal x-ray film (AXR) showed gross dilatation of proximal intestinal bowel loops with absent distal gas highly suspicious of proximal jejunal atresia (Fig. 2). There were no other co-associated anomalies detected.
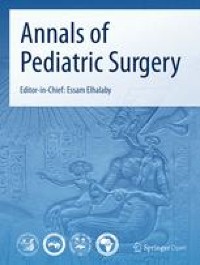
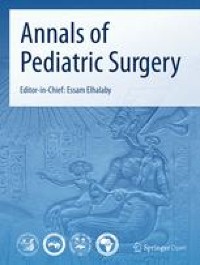
Fig. 1
Prenatal ultrasound image. Prenatal ultrasound image showing a “triple-bubble sign” in a 30-week fetus with mild maternal polyhydramnios
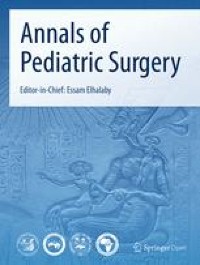
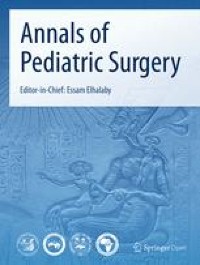
Fig. 2
Postnatal x-ray film (AXR). Postnatal x-ray film showing gross dilatation of the proximal bowel with an absent distal gas pattern — “triple-bubble sign”
An orogastric tube yielded 30 ml of dark bile content. After IV fluid resuscitation and newborn stabilization, an operation was scheduled on the 2nd day of life. Intraoperative findings showed a proximal high type 1 jejunal atresia located critically at the DJ flexure with some 4:1 disproportionate discrepancy (Fig. 3).
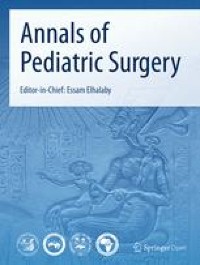
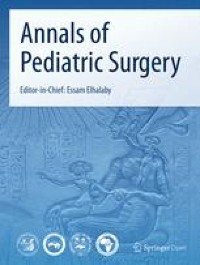
Fig. 3
Intraoperative photograph. Intraoperative photograph demonstrating a high type 1 jejunal atresia. Stay sutures are anchored at the proximal jejunum (*) just immediately below the duodenojejunal flexure (DJFX). Distal jejunum (J) is highlighted below the atretic site (a)
Operative techniqueWe undertook a very limited delicate mobilization of the proximal 4th part of the duodenum creating a transverse incision at this point where a membrane luminal obstruction was identified. Bile together with air bubbles were noted in the gut lumen which confirmed patency of the upstream proximal duodenum. Noting the appreciable size discrepancy and very high location of the gut atresia which would make further mobilization hazardous, we undertook a longitudinal incision in the distal proximal jejunum (Fig. 4) to construct a Kimura jejunojejunostomy primary anastomosis. The anastomosis was successfully completed using interrupted serial 5-0 PDS sutures. No other distal intestinal atresia lesions were evident.
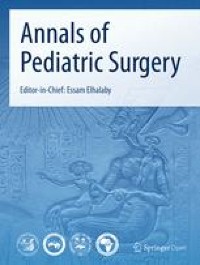
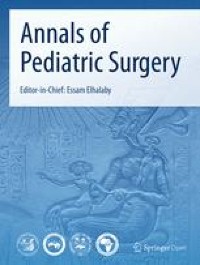
Fig. 4
Illustration of the operative procedure. a Significant size discrepancy between the proximal and distal bowel segments just below the DJ flexure (DJFX). b, c Creation of a transverse incision in the dilated obstructed proximal bowel with a longitudinal incision placed in the adjacent site distal jejunum to create a Kimura primary diamond-shaped anastomosis (d, e)
Post-operative aftercare and follow-upThe infant made a rapid uneventful postoperative recovery. Total parenteral nutrition (TPN) was prescribed in anticipation of significant bowel dysmotility and delayed enteral feeding. We initiated enteral feeding on day 7 post-operatively. Time to then achieve full-enteral feeding was 7 days with a total hospital stay of 24 days. At hospital clinic visits 1 and 3 months after discharge the baby was thriving with body weight (BW) and head circumference (HC) recorded on the P50 centile growth charts. The patient tolerates full oral feeding very well.
Comments (0)