
Remember me









Low tibial osteotomy (LTO) with a medial opening wedge is a useful and proven joint salvage procedure to realign ankle joint with correction of the varus deformity and redistribute weight bearing on the ankle for varus tilted ankle arthritis.
A lateral hinge fracture of the LTO is defined as a fracture, and disruption of the lateral cortex occurs during the medial opening process of the LTO because the lateral cortex acts as a fulcrum with the osteotomy site opening. Compared with numerous previous studies focusing on the lateral hinge fracture associated with medial opening wedge high tibial osteotomy (HTO),1–3 a hinge fracture during LTO has not yet been widely discussed. However, in our clinical experience, hinge fracture during LTO was inevitable as the degree of medial opening increased compared with that of HTO. Moreover, a hinge fracture could distract the distal fragment simultaneously with the medial opening process, resulting in the osteotomy site widening rather than valgization of the distal fragment (Fig. 1).
 FIGURE 1:
FIGURE 1: A lateral hinge fracture during the low tibial osteotomy. A hinge fracture during low tibial osteotomy can distract the distal fragment with the medial opening process, resulting in the osteotomy site widening rather than valgization of the distal fragment.
Therefore, here, we present a simple but effective technical tip to prevent hinge fractures or inhibit further displacement when a lateral hinge fracture occurs during LTO. This study was conducted after the principles of the Declaration of Helsinki. Furthermore, written informed consent was obtained from all enrolled patients. The Inje University Ilsan Paik Hospital ethics review committee approved this study.
TECHNIQUEUnder general or spinal anesthesia, a pneumatic tourniquet on the distal thigh was inflated with the patient in the supine position. An open or arthroscopic examination of the medial ankle joint with synovectomy was conducted. During an open examination, multiple drillings were performed on the cartilage-denuded medial talar dome or medial gutter, whereas the microfracture procedure was performed through the arthroscopic approach. Subsequently, a 4 to 5 cm longitudinal incision was made on the medial supramalleolar area at the osteotomy site, starting 5 cm proximal to the joint line. A 1.6 mm Kirschner wire (K-wire) was fixed from the medial to the lateral aspects along the imaginary oblique osteotomy line under fluoroscopy. The osteotomy line ended toward the proximal 1/3 of the syndesmosis (proximal syndesmotic tibial osteotomy). Next, we estimated the hinge point when a medial osteotomy site was opened (Fig. 2). After a 2 cm vertical incision accompanied by soft tissue dissection at the estimated hinge point, a 1.6 mm K-wire was inserted from 1 cm proximal to the estimated hinge point, traversing distally across the hinge point until reaching the subchondral bone of the tibial plafond. The angle between this K-wire and the anterior tibial surface ranged from 30 to 40 degrees. To enhance the fixation stability, the adoption of bi-cortical K-wire fixation could be contemplated, wherein a more vertically oriented trajectory towards the anterior cortex of the tibia is used to engage and secure the posterior cortex of the tibia.
 FIGURE 2:
FIGURE 2: Kirschner wire fixation to minimize the effect of hinge fracture. After estimating the hinge point before medial osteotomy, a 1.6 mm K-wire was inserted from 1 cm proximal to the estimated hinge point, traversing distally across the hinge point until reaching the subchondral bone of the tibial plafond. During tibial osteotomy, we avoided complete tibial cutting to the lateral cortex by stopping the osteotomy when the oscillating saw reached the K-wire. After locking the plate and screw fixation, an additional K-wire can be fixed optionally in a direction similar to the preceding K-wire to secure the hinge site more firmly.
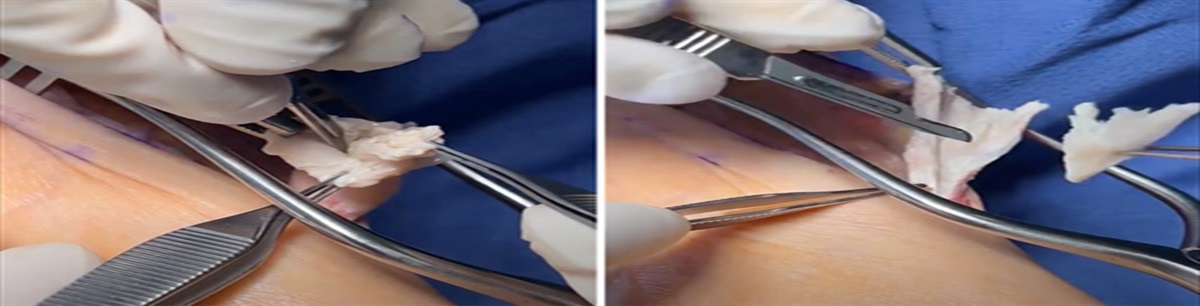
We performed fibular oblique osteotomy before tibial osteotomy to prevent tibial hinge fracture with medial opening as we believed that the load from the valgization force would be entirely applied to the tibia with an intact fibula. Next, tibial osteotomy was performed using an oscillating saw along the first temporary K-wire on the imaginary osteotomy line. Complete tibial cutting to the lateral cortex was avoided by stopping osteotomy when the oscillating saw reached the second K-wire. The osteotomy site was opened, and the resulting gap was filled with a tricortical autograft from the anterosuperior iliac spine of the pelvic bone with an allograft bone block or a metal block. The autograft or bone/metal block width to maintain the osteotomy opening was determined intraoperatively when preoperatively planned correction was achieved under fluoroscopy (the goal of corrected tibial anterior surface angle: 92 to 93 deg). Subsequently, a locking plate and screws were fixed to firmly secure the tibial and fibular osteotomy sites. Optionally, an additional 1.6 m K-wire can be fixed in a similar direction to the protective K-wire to secure the hinge site more firmly. When the surgeon performs this optional K-wire fixation, it is crucial to fix the wire bi-cortically same as the prior K-wire.
However, the K-wires used to hold the hinge site can be fixed either proximal to the distal (to the osteotomy line) or distal to the proximal. When the surgeon plans to perform distal syndesmotic tibial osteotomy, the K-wire starting from the distal part would be technically easier because the adequate room for wire fixation at the distal part of the tibial osteotomy site is narrow (Fig. 3). Moreover, surgeons can decide whether to leave or remove the K-wires after plate fixation at the osteotomy site. However, we recommend leaving the K-wires until the osteotomy site is united because these wires may add stability at the hinge point.
 FIGURE 3:
FIGURE 3: An application of the technique in distal syndesmotic low tibial osteotomy. When the surgeon plans to perform a distal syndesmotic tibial osteotomy, Kirschner wire from the distal part is technically easier because the adequate room for wire fixation at the distal part of the tibial osteotomy site is narrow.
Postoperatively, weight bearing was prohibited in a below-knee cast for 6 weeks. Subsequently, partial weight bearing without a cast was permitted, and full weight bearing was allowed 3 months postoperatively when the adequate radiographic bony union had been achieved.
EXPECTED OUTCOMESWith our technique, surgeons can expect to minimize or prevent the effect of hinge fractures during LTO for varus tilted ankle arthritis. Although one temporary K-wire can provide sufficient benefit for stable maintenance, we recommend fixing 2 wires and leaving them after plate and screw fixation to ensure secure maintenance of a lateral hinge point until osteotomy site union is achieved.
Although numerous studies on osteotomy around the knee joint have already been conducted, to the best of our knowledge, only a few researchers have focused on the role and radiographic characteristics of hinge fractures during osteotomy at the distal tibial area. Although the exact incidence and risk factors of lateral hinge fractures during LTO remain unknown, an interesting study by Park et al4 revealed that lateral hinge fractures were observed in 48.7% of LTO cases on plain radiographs. However, the incidence increased with computed tomography (61.5%). They insisted that postoperative computed tomography was suitable when lateral hinge fractures were unclear on plain radiographs, although the number of participants was too small (39 patients) to provide concrete evidence. In our clinical experience with more than 200 cases of LTO, a lateral hinge fracture during LTO was inevitable in most cases when the degree of the medial opening was more than 7.5 mm, with or without fibular osteotomy. Therefore, future studies focusing on the incidence of lateral hinge fractures and the risk factors influencing lateral hinge fractures, including the association between the degree of opening, are highly recommended to obtain more scientific evidence.
In addition to reducing the degree of medial opening, several factors should be considered to prevent lateral hinge fractures during LTO. Regarding the location of tibial osteotomy, Kim et al5 proposed that when fibular osteotomy is not performed, intra-syndesmotic LTO should be considered because lateral hinge fractures are less likely with soft tissue support. We completely agree that lowering the location of the tibial osteotomy can be adequate consideration for preventing lateral hinge fractures. In addition, we believe that preceding fibular osteotomy without fixation before tibial osteotomy can prevent lateral hinge fractures when the conventional proximal syndesmotic LTO is performed as the fibula plays a restricting role. In our opinion, as the fibula would resist as a buttress against the medial opening process, freeing the fibula before tibial osteotomy may be another adequate consideration to prevent hinge fractures. Compared with the role of the fibula in HTO, that in LTO would be substantially different with respect to the lateral hinge fracture prevention. Therefore, it is also recommended that future studies focus on this issue.
COMPLICATIONSComplications related to the application of protective K-wire fixation were not observed including osteotomy site nonunion, delayed union or superficial/deep surgical site infection. However, surgeons should be aware of the possible injury of medial or intermediate dorsal cutaneous branch of superficial peroneal nerve as the incision is performed nearby the course of these branches. Furthermore, it is worth considering to fix the K-wires bi-cortically for firmer fixation and surgeons should avoid tilting the K-wires too medially because neurovascular structures on the posteromedial corner of distal tibia can be damaged.
REFERENCES 1. Takeuchi R, Ishigawa H, Kumagai K, et al. Fractures around the lateral cortical hinge after a medial opening-wedge high tibial osteotomy: a new classification of lateral hinge fracture. Arthroscopy. 2012;28:85–94. 2. Lee BS, Jo BK, Bin SI, et al. Hinge fractures are underestimated on plain radiographs after open wedge proximal tibial osteotomy: evaluation by computed tomography. Am J Sports Med. 2019;47:1370–1375. 3. Lee SS, Celik H, Lee DL. Predictive factors for and detection of lateral hindge fractures following open wedge high tibial osteotomy; plain radiography versus computed tomography. Arthroscopy. 2018;34:3073–3079. 4. Park YH, Lee HJ, Choi JW, et al. Value of postoperative computed tomography for the diagnosis of lateral hinge fracture in medial opening-wedge supramalleolar osteotomy. Arch Orthop Trauma Surg. 2023;143:1379–1385. 5. Kim HJ, Yeo ED, Rhyu IJ, et al. Changes in ankle joint motion after supramalleolar osteotomy: a cadaveric model. BMC Musculoskelet Disord. 2017;18:389.
Comments (0)