
Remember me









Blount disease is commonly related to an intrinsic, idiopathic defect in the posteromedial proximal tibial physis resulting in progressively increasing bowing of the leg, in-toeing in addition to lateral knee thrust with lateral collateral ligament, and posterolateral corner laxity, also known as pathologic tibia vara.1,2
Two main options are commonly described in the literature for treatment:
The first option is osteotomy: acute or gradual corrective osteotomy and is the main standard treatment for angular deformity, second option is epiphysiodesis and guided growth surgeries either by staples or guided growth plate of the tibia.3
Our rationale is that Blount disease has a bony and ligamentous laxity element of the lateral collateral ligament that can be corrected simultaneously through hemiepiphysiodesis of the tibia and epiphysiodesis of proximal fibula physis by cannulated screws. This was specially directed to adolescent Blount disease to solve the problem of lateral collateral ligament laxity by addressing the lateral compartment. The other options of treatment do not address the lateral compartment and lateral collateral ligament laxity.
The study aims to assess the safety and the efficacy of adding the fibular guided growth to the well-known technique of tibial hemiepiphysiodesis in the treatment of late-onset Blount disease.
PATIENTS AND METHODSThis is a retrospective study that is conducted on human participants with the approval of the Human Research Ethical Committee.
This study comprises 23 limbs with a diagnosis of pathologic tibia vara, which was treated between 2010 and 2017 and followed up for 2 to 6 years (mean, 4.13 y). Nineteen of the patients were males whereas 4 of them were females. Ages ranged from 9 to 13 years (mean, 11.26) with all patients having a late-onset type Blount disease (adolescent Blount). There were 16 limbs with langenskoild type 3 and 7 limbs with langenskoild type 4. All patients were before stage tanner 2 of maturity on clinical examination and had a minimum of 2 years of growth before physeal closure as evidenced by hand x-rays.
Patients with metabolic and neurological disorders, skeletal dysplasia, and previous trauma, were not considered for inclusion. All patients were followed in an outpatient setting by a single surgeon.
We used a guided growth technique for the gradual correction of the varus deformity and lateral collateral ligament laxity. We use a cannulated screw of 6.5 mm for hemiepiphysiodesis of the lateral side of the proximal tibial physis whereas a cannulated 4 mm screw was used for fibular epiphysiodesis.
The whole limb is draped by betadine then the knee is flexed 90 degrees to facilitate imaging. For the tibial screw we either put the wire in antegrade or retrograde so that the wire is central in lateral view and directed to the lateral epiphysis. This is ensured by anteroposterior and lateral views. If we use the antegrade method, we pass the wire through the medial tibia and make a small incision of about 0.5 cm. Then we drill for the screw in a retrograde manner from the medial side of the tibia and we insured that we did not penetrate the articular surface by image intensifier through 20-degree flexion of the knee. The length of the screw is justified, then a 6.5 fully threaded screw is introduced and again we ensured that the articular surface was not penetrated by the image intensifier.
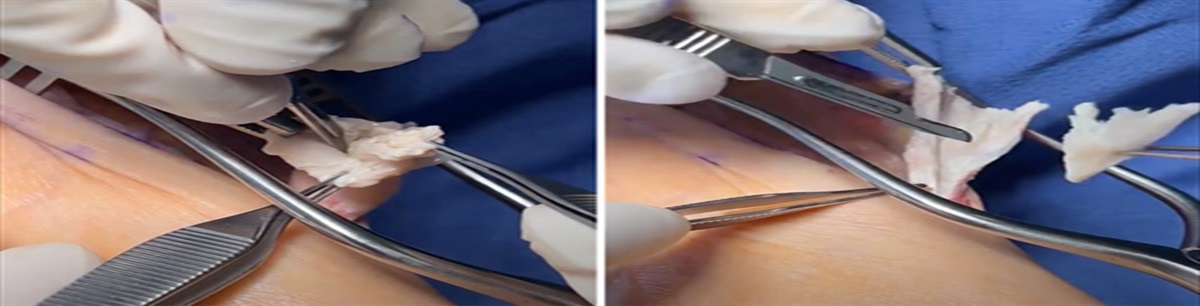
Another fully threaded cannulated cancellous 4 mm screw is inserted traversing the proximal fibular epiphysis. The latter screw is introduced through the fibular head and passes with a distal trajectory, again, under fluoroscopic guidance. The course of the common peroneal nerve is identified by surface anatomy, which in combination with fluoroscopic guidance and adequate caution prevented any injury to the nearby nerve. (Figs. 1 and 2)
 FIGURE 1:
FIGURE 1: Intraoperative surgical photos and radiograph of the technique of tibial screw insertion.
 FIGURE 2:
FIGURE 2: Intraoperative photos and radiograph showing the application of the fibular screw.
Pre and postoperative radiographs were evaluated to determine the accuracy of correction using standard metrics; full-length, weight-bearing, anterior-posterior radiographs of the lower extremities were evaluated for angular deformity, as well as proximal tibial and physeal morphology to determine the stage of the disease. Measurement of the mechanical axis deviation, medial proximal tibial angle (MPTAm), lateral distal femoral angle (LDFAm), and joint line congruence angle (JLCA) preoperative, and at 2 years follow-up were used as indicators of correction of the varus deformity. The mechanical axis was evaluated by drawing a line from the center of the femoral head to the talus, traversing the knee.4
Statistical AnalysesData were analyzed using IBM SPSS Statistics software, version 21 (IBM Corp.). Continuous data were expressed as mean ± SD. Paired sample t test of significance (P value) was used when comparing related samples. The P value was considered significant when <0.05.
Lateral ligamentous laxity was assessed clinically by stress varus test of the knee, as well as radiographically by comparing the JLCA in long plain x-ray film in supine and standing positions to assess the added ligamentous laxity.
Immediate mobilization and full-length weight-bearing were encouraged after surgery. No casting or bracing was utilized postoperatively as the pain was minimal and was easily controlled by analgesics to allow an early range of motion as well. Patients were subsequently evaluated in a clinical setting.
RESULTSPatients were followed up for an average duration of 4.13 years. There was a statistically significant improvement (P value: 0.032) of the radiographic parameters in the form of MPTAm, JLCA, and LDFAm. Details are discussed in the statistical disclosure control (Table 1).
TABLE 1 - Patient’s Demographics and Deformities Preoperative mean value (degrees) Postoperative value (degrees) P MPTAm 73.22. SD: 3.529 87.78. SD: 1.594 0.032 Supine JLCA 7.52. SD: 1.163 1.2. SD: 0.926 0.027 Standing JLCA 8.2. SD: 1.17 1.3. SD: 0.94 0.030 LDFAm 90.87 SD: 1.29 88.26. SD: 1.573 0.031Preoperative and postoperative mean values of the angles measured in the study.
JLCA indicates joint line congruence angle; LDFAm, lateral distal femoral angle; MPTAm, medial proximal tibial angle.
The mean preoperative MPTAm was 73.22 degrees (range, 66 to 78 degrees SD: 3.529 degrees) was corrected to a final postoperative mean of 87.78 degrees (range, 85 to 90 degrees SD: 1.594 degrees). The mean preoperative supine JLCA was 7.52 degrees (range, 4 to 9 degrees, SD: 1.163 degrees), mean preoperative standing JLCA was 8.2 degrees. While the supine postoperative JLCA was corrected to a mean of 1.2 degrees (range, 0 to 3 degrees, SD: 0.926 degrees) and the mean standing postoperative JLCA was corrected to 1.3 degrees.
The mean preoperative LDFAm was 90.87 degrees (range, 89 to 94 degrees, SD: 1.29 degrees) and was corrected to a final postoperative mean of 88.26 degrees (range, 85 to 90 degrees, SD: 1.573 degrees).
All patients were clinically and radiographically completely corrected without complications, except 1 patient who experienced surgical site superficial infection, was treated medically with antibiotics, and followed up till complete correction occurred.
DISCUSSIONTreatment of Blount disease aims to correct the mechanical axis deviation, so all deformities (tibial torsion, varus, and genu procurvatum) have to be corrected.5,6 This, in turn, prevents the complications that may occur as early onset degenerative joint disease.7,8
In our study, when we stop proximal fibular growth, we assume that the fibula is still attached to the distal tibiofibular joint and the tibia continues to grow distally as well as proximal medial tibial epiphysis.
That could be acting as a gradual tensioning mechanism of the lateral collateral ligament because the fibula is getting shorter in relation to the tibia. we found that this technique is a relatively safe and effective first-line treatment in this group, especially given the potential complications associated with high tibial osteotomy or physical ablation as a common peroneal nerve injury.
Permanent methods of guided growth act through the destruction of the lateral hemiepiphysis to stop its growth relative to the compromised medial epiphysis, thus achieving gradual correction up to normalization of the mechanical axis.5
The partial physeal ablation method has the disadvantages of being permanent and requiring exact timing for surgery. Staples, transphyseal screws, and 8-plate have the theoretical advantage of being reversible. Transphyseal screws risk growth disturbance because crossing physis and staples have some potential complications such as breakage, migration, and difficulty of removal.9
Acute or gradual correction of the varus deformity has been achieved frequently through a proximal osteotomy of the tibia with several types of procedures as osteotomies and fixation methods, with the disadvantages of longer operative time, more blood loss, delayed weight-bearing, delayed union, neurological injury, compartment syndrome or malunion.10–12 A simpler technique that utilizes correction by guided growth of the proximal tibial physis seems encouraging.13
Temporary epiphysiodesis depends on the Hueter-Volkmann law14 where the compression of the lateral hemiepiphysis leads to hindered growth on that side, again, with the eventual correction of the mechanical axis by the unrestricted medial physeal growth correcting angular deformities in children.
Methods of temporary epiphysiodesis include; staples, tension band plates, and percutaneous transphyseal screws (PETS).15
PETS have the advantages of being a minimally invasive operation with a very short intraoperative time, little blood loss, little to no hematoma formation as well as possible weight-bearing from the first day postoperatively thereby eliminating the need for immobilization. There is no need for the permanent destruction of the growing child’s epiphysis. However regular follow-up is essential as it is a temporary method of epiphysiodesis.16
Moreover, PETS have been found to have a low risk of implant-related complications and are not adversely affected by the high prevalence of obesity among Blount patients, unlike the tension band plate, in which the risk of breakage increases in obese patients.16
Woo and colleagues included 25 patients with idiopathic genu varum (50 lower limbs) who underwent percutaneous lateral hemiepiphysidesis on the proximal lateral tibia for a varus angular deformity. The amount of coronal deformity of the lower limb was significantly improved, as compared with the preoperative values. The coronal deformity of the knee joint with hip-knee-ankle angles was assessed. The median value of the percent ratio of the correction of the hip-knee-ankle angle was 60.0% (interquartile range, 50.0% to 71.4%).17
Our technique depends on the utilization of PETS for its advantages together with adding another transphyseal proximal fibular screw, which addresses the lateral ligamentous laxity preventing the growth of the proximal physis of fibula thereby; preventing the development of any further laxity during the course of gradual modification of the mechanical axis through guided growth.
Castañeda and colleagues condemned the use of hemiepiphysiodesis in adolescent Blount disease in a series of 35 patients. It should be noted that their study evaluated the success of temporary and permanent epiphysiodesis.18
In our study, there are no major complications as common peroneal nerve injury, wound dehiscence, deep infection, reactive synovitis, hardware failures, and need for further osteotomy with near or complete correction in patients age the age between 13 and 18 years old using the cannulated screws. The success is clear with the significant improvement of the JLCA in both the supine and standing positions, confirming ligamentous laxity improvement.
In our study, we improved the results by adding epiphysiodesis of the fibula together with hemiepiphysiodesis of the lateral part of the tibia to solve the problem of lateral collateral ligament laxity by addressing the lateral compartment. This is controlled through the differential growth between the tibia and fibula resulting in gradual correction of the laxity. And to our knowledge, this type of surgery is not described in the literature.
Limitations of our study include the absence of a control group and short follow-up, so we consider further research to compare our technique with other techniques and a longer follow-up period.
Fibular guided growth surgery in addition to lateral proximal tibia epiphysiodesis addressed the bony and ligamentous pathology having the advantage of being minimally invasive, having no dissection, low risk of permanent perichondrium, or periosteal damage, and improving the corrective power of hemiepyphysiodesis of the lateral compartment of the knee with impressive results in Blount disease cases.
REFERENCES 1. Bowen RE, Dorey FJ, Moseley CF. Relative tibial and femoral varus as a predictor of progression of varus deformities of the lower limbs in young children. J Pediatr Orthop. 2002;22:105–111. 2. Heflin JA, Ford S, Stevens P, et al. Guided growth for tibia vara (Blount’s disease). Medicine. 2016;95:41. 3. De Pablos J, Arbeloa-Gutierrez L, Arenas-Miquelez A. Update on treatment of adolescent Blount disease. Curr Opin Pediatr. 2018;30:71–77. 4. Hsu RWW, Himeno S, Coventry MB, et al. Normal axial alignment of the lower extremity and load-bearing distribution at the knee. Clin Orthop Rel Res. 1990;255:215–227. 5. Thompson GH, Carter JR. Late-onset tibia vara (Blount’s disease). Clin Orthop Relat Res. 1990;255:24–35. 6. Cook SD, Lavernia CJ, Burke SW, et al. A biomechanical analysis of the etiology of tibia vara. J Pediatr Orthop. 1983;3:449–454. 7. Stanitski DF, Stanitski CL, Trumble S. Depression of the medial tibial plateau in early-onset Blount disease: myth or reality? J Pediatr Orthop. 1999;19:265–269. 8. Brooks WC, Gross RH. Genu varum in children: diagnosis and treatment. J Am Acad Orthop Surg. 1995;3:326–335. 9. Métaizeau JP, Wong-Chung J, Bertrand H, et al. Percutaneous epiphysiodesis using transphyseal screws (PETS). J Pediatr Orthop. 1998;18:363–369. 10. Alekberov C, Shevtsov VI, Karatosun V, et al. Treatment of tibia vara by the Ilizarov method. Clin Orthop Relat Res. 2003;409:199–208. 11. Stanitski DF, Srivastava P, Stanitski CL. Correction of proximal tibial deformities in adolescents with the T-Garches external fixator. J Pediatr Orthop. 1998;18:512–517. 12. Payman KR, Patenall V, Borden P, et al. Complications of tibial osteotomies in children with comorbidities. J Pediatr Orthop. 2002;22:642–644. 13. Oto M, Yilmaz G, Bowen JR, et al. Adolescent Blount disease in obese children treated by eight-plate hemiepiphysiodesis. Eklem Hastalik Cerrahisi. 2012;23:20–24. 14. Stokes IA. Mechanical effects on skeletal growth. J Musculoskelet Neuronal Interact. 2002;2:277–280. 15. Ghanem I, Karam JA, Widmann RF. Surgical epiphysiodesis indications and techniques: Update. Curr Opin Pediatr. 2011;23:53–59. 16. Murphy RF, Pacult MA, Barfield WR, et al. Hemiepiphyseodesis for Juvenile and adolescent tibia vara utilizing percutaneous transphyseal screws. J Pediatr Orthop. 2017;40:17–22. 17. Woo K, Lee YS, Lee WY, et al. The Efficacy of percutaneous lateral hemiepiphysiodesis on angular correction in idiopathic adolescent genu varum. Clin Orthop Surg. 2016;8:92–98. 18. Castañeda P, Urquhart B, Sullivan E, et al. Hemiepiphysiodesis for the correction of angular deformity about the knee. J Pediatr Orthop. 2008;28:188–191.
Comments (0)