
Remember me









Patellar tendon ruptures are a relatively infrequent yet disabling injury that usually occurs in active patients under the age of 40. Delays in operative management can pose a significant challenge to the treating surgeon, as chronic ruptures of greater than 2 weeks have been shown to have poorer results compared with acute tears.1 In acute tears of less than 2 weeks, direct end-to-end repair is often achieved in operative treatment; however, this is rarely feasible in chronic tears due to tear retraction, scarring, and degeneration of surrounding tissues.2 In the case of a chronic tear where direct repair is not possible, the tendon is often reconstructed using either allografts or autografts. As chronic patellar tendon tears are rare, there is no consensus in the literature regarding operative techniques, and many techniques have been described utilizing hamstring and Achilles tendon autograft or allograft, among other options.3 We describe our surgical technique for the reconstruction of chronic patellar tendon rupture using semitendinosus allograft passed through a longitudinal trans-osseous patellar tunnel with a proximal split to recreate both the medial and lateral retinaculum.
TECHNIQUEGeneral anesthesia is typically used at our institution, though there is nothing that would prevent this technique from being used with spinal anesthesia. Before draping, a perfect lateral of the contralateral knee can be used to estimate patellar height. A nonsterile tourniquet is applied, and the surgical extremity is prepped and draped in the typical fashion with the patient supine. It is part of the senior author’s practice to perform these open procedures with a tourniquet. We do recognize the existence of tourniquet-based pain, and so we set the tourniquet to 275 mm Hg and make every effort to minimize the time during which the tourniquet is inflated. The tourniquet is used to maximize operative visualization so that the procedure can be done in the most efficient manner possible.
A padded cushion may be placed underneath the leg to improve the ease of obtaining fluoroscopic imaging. A midline incision is utilized, extending from just proximal to the superior patellar pole and extending distally to the tibial tubercle. Sharp dissection is carried out with full-thickness flaps developed medially and laterally to identify the degree of injury to the medial and lateral retinaculum. After this, the patellar tendon injury is identified, and the native tendon remnant is split in the midline in line with its fibers down to the level of the tibial tubercle. The tendon insertion on the tubercle is elevated just enough to expose the site for the allograft socket to be drilled. A 6 mm socket is drilled to a sufficient depth to allow for interference screw fixation. The previously prepared, whip-stitched end of a nonirradiated semi-tendinosis allograft is then shuttled into the socket and fixated in place with an interference screw. After this, attention is turned back to the inferior patellar pole. All residual tissue is debrided back to the bleeding bone, and the central portion is identified for placement of the patellar tunnel. A guide wire is placed in a retrograde fashion, and its position in the center of the patella is confirmed in both the AP and lateral views with care to respect the articular surface (Fig. 1). Superiorly, its exit point from the superior pole of the patella is identified and the quadriceps tendon is split with bovie electrocautery in line with its fibers back to identify the bony exit point. This is then over-reamed with the appropriately sized reamer, typically 6 to 6.5 mm. The free end of the graft is then shuttled through the tunnel (Fig. 2). The graft is then tensioned by pulling it directly distal over the anterior aspect of the patella with the help of an assistant and the position of the patella confirmed both visually and fluoroscopically to recreate appropriate patellar height. The graft is then fixated at the distal and proximal aspect with interference screws in a retrograde and antegrade fashion, respectively (Fig. 3). After this, the remaining proximal graft is split in half in line with its fibers. It is folded back on itself both medially and laterally around the border of the patella and sequentially sutured into place along the medial and lateral aspects of the patella with a braided absorbable suture to augment the repair of the retinaculum. At the inferior pole of the patella, the 2 limbs are sutured into the previously fixated allograft limb, thus creating a three-stranded reconstruction (Fig. 4). The native tendon is then closed over the allograft and incorporated into the repair with horizontally placed continuous sutures (Fig. 5). In regards to suture, 0-vicryl is used to incorporate the split portions of the graft into the medial and lateral retinaculum for augmentation purposes. 0-vicryl is also used to incorporate the graft into the patellar tendon. 2-0-Vicryl is used for the subcutaneous tissue, followed by 3-0 Monocryl for the skin. Every patient who undergoes this procedure then has postoperative clinic follow-up appointments scheduled at 2 weeks, 6 weeks, 12 weeks, 6 months, and 1 year.
 FIGURE 1:
FIGURE 1: AP and lateral fluoroscopic images showing the center-center orientation of the guide wire used to create the path for the graft tunnel.
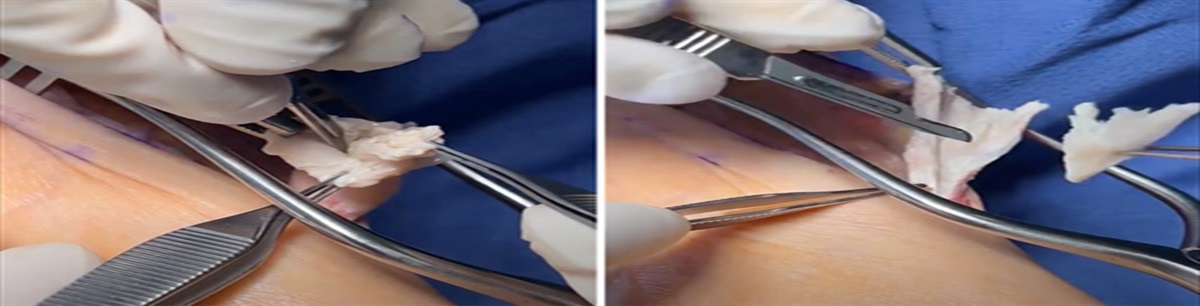
 FIGURE 2:
FIGURE 2: The allograft has been passed through the patellar tunnel in a retrograde fashion.
 FIGURE 3:
FIGURE 3: Once the graft has been adequately tensioned, it is fixated at the distal and proximal aspects using interference screws.
 FIGURE 4:
FIGURE 4: At this point, the graft has been sutured into place along the medial and lateral aspects of the patella. Next, it will be sewn into the remnants of the native patellar tendon with a horizontally placed suture to maximize fixation strength.
 FIGURE 5:
FIGURE 5: Final representation of the graft after it has been sutured into place along the medial and lateral aspects of the patella with braided absorbable suture to reinforce the retinaculum. Note that the native tendon is also sewn into the allograft with a horizontally placed suture.
EXPECTED OUTCOMESAs of January 1, 2023 and dating back to January 1, 2016, this technique has been used on 11 patients, 1 of which required the reconstruction of bilateral patellar tendon ruptures. Outcomes are assessed through physical exams conducted at follow-up appointments. In addition, radiographs are obtained at each follow-up appointment and compared with intraoperative fluoroscopic images to assess for interval development of patella alta or baja.
The advantages this technique provides over previously described alternatives are 2-fold. First, this technique utilizes a vertically oriented tunnel in the patella. This helps to minimize the risk of a transverse fracture of the patella. In addition, this allows for optimal tensioning of the patella in cases of chronic patella alta, helping to minimize the risk of iatrogenic patella baja or persistent alta. Secondly, this technique allows for the reconstruction of both the medial and lateral retinaculum, which improves the strength of the overall construct without the need for using an additional graft or anchor fixation. In addition, while we advocate a conservative stepwise progression of activity, the robust fixation of this technique is somewhat protective in the setting of decreased patient compliance and allows for an early range of motion.
COMPLICATIONSWhile thus far in the senior author’s practice, there have not been any loss of fixation or need for revision, placement of a trans-patellar tunnel does create a theoretically increased risk of intraoperative or postoperative fracture. However, the vertical nature of the tunnel, in this case, would be expected to minimize the risk of an extensor mechanism-disrupting transverse fracture. Careful attention to the position of the guide wire placement and fluoroscopic confirmation of the guide wire position before reaming can also help to minimize the fracture risk. Iatrogenic baja or alta could also be a complication with this technique. However, the vertical nature of the tunnel and the use of fluoroscopy has allowed for simple tensioning and fixation in an anatomic position. Care to make sure the patella is at an appropriate height before final fixation is critical. Obtaining a perfect lateral fluoroscopic view of the contralateral knee before draping can be a useful aid in minimizing the risk of iatrogenic baja or alta. Finally, postoperative stiffness is a concern with prolonged immobilization after repair or reconstruction of extensor mechanism disruptions. The robust fixation with this technique allows for the early protected progression of motion to help mitigate this risk. In summary, this technique creates a robust, reproducible, and straightforward manner of treating these injuries without an increase in postoperative complications.
REFERENCES 1. Siwek CW, Rao JP. Ruptures of the extensor mechanism of the knee joint. J Bone Joint Surg Am. 1981;63:932–937. 2. Samagh SP, Huyke FA, Buchler L, et al. Treatment of a neglected patellar tendon rupture with a modified surgical technique: Ipsilateral semitendinosus autograft reconstruction with suture tape augmentation. Case Rep Orthop. 2018;2018:2037638. 3. Ginesin EZ, Wojnowski NM, Patel RM. Patellar tendon reconstruction for a chronic extensor mechanism deficit using an achilles tendon allograft with hamstring autograft and suture augmentation. Arthrosc Tech. 2020;9:e469–e475.
Comments (0)