
Remember me









Soft tissue sarcomas (STSs) comprise a heterogenous group of rare and aggressive tumors arising from mesenchymal tissues that can occur anywhere in the body.1 Although relatively rare, accounting for <1% of all malignant tumors, ∼10% of patients have metastasis present at diagnosis and nearly 50% of the patients with STS will ultimately develop distant metastases.2 Treatment with curative intent of STSs consists of wide resection with negative margins and typically neoadjuvant and/or adjuvant radiation therapy to decrease the risk of local recurrence. While the average size of a STS at presentation is 10 cm, ∼10% of patients present with large tumors that are >20 cm.3 Depending on the anatomic location, larger tumor size can make margin negative resection more technically challenging (Fig. 1). In some cases, large sarcomas or those that have been treated with neoadjuvant radiation may contain an internal fluid cavity as a result of tissue necrosis or hemorrhage.4 The added mass effect from a sizeable internal fluid cavity can complicate safe dissection around the tumor, thereby increasing the risk of positive margins. Unexpected positive margins after STS resection have been associated with increased local recurrence rates as high as 35%, an almost 4-fold increase from that expected with negative margins, and a rate of future metastatic spread near 49%.5 In addition, in this setting, unintentional rupture of the fluid cavity and tumor spillage results in a grossly contaminated resection bed. This paper will outline a technique for controlled intraoperative decompression of soft tissue tumors with internal fluid cavities, which can facilitate dissection around the tumor and improve visualization during resection while simultaneously decreasing risk of inadvertent rupture.
 FIGURE 1:
FIGURE 1: Axial imaging positron emission tomography/computed tomography of high-grade neoplasm of the lower extremity with associated fluid cavity exhibiting mass effect on adjacent critical structures.
TECHNIQUEPreoperative advanced imaging of the mass is recommended to best characterize the local anatomic and adjacent neurovascular structures, as well as the contents of any internal fluid cavity. Magnetic resonance imaging with and without contrast is the imaging study of choice to obtain, however, computed tomography scan with contrast or a positron emission tomography/computed tomography scan can also provide useful information (Fig. 1). Intraoperatively, a standard oncologic approach and dissection are performed based upon the anatomic location of the tumor. Once a superficial portion of the soft tissue mass has been exposed for decompression, a 0-silk suture is placed in purse string fashion in the tissue adjacent to the tumor capsule. A scalpel is then used to penetrate the capsule within the bounds of the purse string suture. Next, an 18 or 22 Fr chest tube attached to suction is inserted into the internal fluid cavity (Fig. 2). Note, the use of a chest tube is recommended over a standard Yankauer suction device due to the propensity of the latter to become clogged with debris. Once sufficient decompression has been performed, the suction device is extracted from the wound, and the purse string suture is tied securely. It is important to note that by function of achieving partial exposure and puncture of the tumor in order allow for decompression, this technique effectively intentionally performs an R1 resection to decrease risk of accidental R2 resection due to accidental spillage and rupture of noncompressed tumors, thus theoretically allowing for a lower, more consistent overall risk of local recurrence.
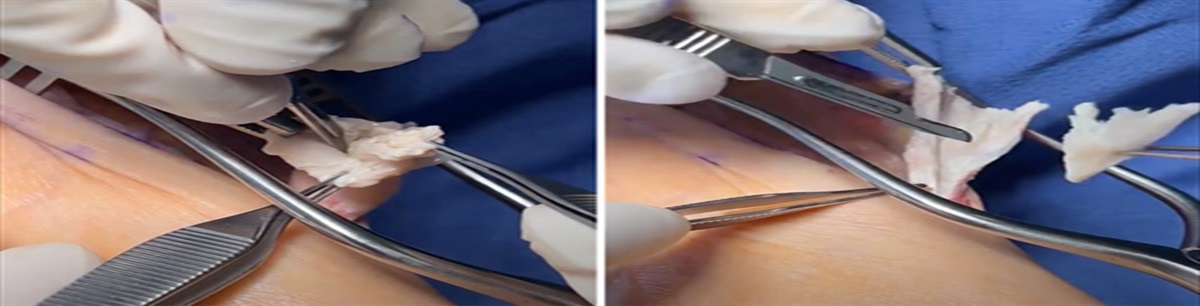
 FIGURE 2:
FIGURE 2: Insertion of chest tube through incision with circumferential purse string suture.
Alternatively, if the fluid cavity is close to the skin surface, decompression can be performed percutaneously before a formal surgical approach. This can be done initially with a large bore needle or through a technique similar to that described above. Subsequently, the skin surrounding the percutaneous approach may be excised en bloc with the tumor.
Before proceeding with en bloc resection of the mass, the field should be thoroughly irrigated with or without use of adjuvant cleaning solutions such as hydrogen peroxide per surgeon preference. At this point, the field may be reprepped in sterile fashion if necessary, and the planned wide resection of the tumor is then performed with improved mobilization and visualization of the tumor and surrounding anatomic structures.
CASE EXAMPLEA 57-year-old morbidly obese male with past medical history of a T4 N0 M0 G3 dedifferentiated liposarcoma of the right lower extremity extending from the knee joint to the hip joint (Fig. 3). Due to the size of the tumor, associated fluid collection, and adjacency to bone and critical structures, this was considered a complex tumor which would entail a resection with high degree of difficulty and a significantly elevated risk of local recurrence even if appropriate R1 or R0 resection was successfully performed.
 FIGURE 3:
FIGURE 3: Clinical photograph of the mass in patient right thigh.
To allow for mobilization of the patient’s tumor away from the femur and femoral neurovascular structures (Fig. 1), the above-described decompressive procedure was performed over the cystic mass through the skin and capsule at the right thigh. A total of 9 L of liquified material and old hematoma were evacuated through the purse string approach which led to decompression of ∼50% of the volume of the tumor. The vastus intermedius, which contained the mass, was dissected circumferentially in its entirety from the hip joint to the knee joint. There was an anticipated focal positive margin along the anteromedial femur after resection, which did not appear to infiltrate the cortex. Saucerization was performed at this location using curettes, followed by cauterization and irrigation with hydrogen peroxide.
The patient experienced delayed wound healing but did not require reoperation. He subsequently underwent targeted adjuvant radiation therapy to the medial aspect of the tumor bed in the right thigh, including the medial cortex of the right femur at the location of previous saucerization. Due to morbid obesity, periosteal stripping, and adjuvant radiation therapy the patient was deemed at high risk for impending pathologic fracture of the femur. Prophylactic intramedullary nailing of the femur was performed without complication 7 months following initial surgery. He developed distant metastasis to the lung 9 months status postresection for which he has received intermittent systemic chemotherapy and focal radiation therapy. On surveillance scans 17 months after initial surgery, there was evidence of cortical disruption and local recurrence at site of right femoral saucerization. This patient, however, remains alive with disease at the time of this description.
COMPLICATIONSIntraoperative spillage can still be a risk with this method if the initial poke-hole incision into the purse string entry is made too large or if inappropriate externally applied pressure is placed on the fluid collection while draining. Leakage may also occur if closure of the purse string suture is inadequate and/or all fluid is not completely drained before closure. These complications can be avoided by careful attention to the size of suction device that will be used for decompression and ensuring the entry incision is no larger than required in addition to reliable closure of the purse string suture and maximal decompression of the fluid cavity. When applicable, draining the tumor percutaneously will provide a more secure closure of this hole and provide less chance of leakage.
EXPECTED OUTCOMESThe suction device decompression technique is expected to improve the safety and feasibility of resection in select large STSs with internal fluid cavities by facilitating dissection around the mass and improving visualization of adjacent neurovascular structures. In addition, drainage of the fluid cavity may reduce the risk of inadvertent rupture and gross tumor spillage. In doing so, preresection decompression can, as illustrated in this technique paper, improve patient safety and facilitate surgical attempts at resecting tumors that had relative contraindications to wide resection or limb salvage. Furthermore, while tumor decompression presents an additional operative step, this technique can reduce overall surgical time.
CONCLUSIONSThe described method for meticulous surgical decompression by closed suction drainage of large intratumoral fluid collections facilitates wide resection of soft tissue neoplasms. This technique provides a safe, simple, and effective method for facilitating STS decompression and resection which has previously not been reported in the orthopedic and surgical oncology literature.
REFERENCES 1. Kneisl JS, Coleman MM, Raut CP. Outcomes in the management of adult soft tissue sarcomas. J Surg Oncol. 2014;110:527–538. 2. Voltan K, Baptista AM, Etchebehere M. Extremities soft tissue sarcomas, more common and as dangerous as bone sarcomas. Rev Bras Ortop (Sao Paulo). 2021;56:419–424. 3. Grimer RJ. Size matter for sarcomas! Ann R Coll Surg Engl. 2006;88:519–524. 4. Mullen JT, Hornicek FJ, Harmon DC, et al. Prognostic significance of treatment-induced pathologic necrosis in extremity and truncal soft tissue sarcoma after neoadjuvant chemoradiotherapy. Cancer. 2014;120:3676–3682. 5. O’Donnell PW, Griffin AM, Eward WC, et al. The effect of the setting of a positive surgical margin in soft tissue sarcoma. Cancer. 2014;120:2866–2875.
Comments (0)