Study Design and Data Source
This retrospective, observational cohort study used COTA’s Real World Evidence (RWE) database, an electronic health records (EHR)-derived, de-identified oncology database [20]. The database includes data from 1.7 million patient records from over 1500 oncologists, of whom approximately 50% are from academic settings and 50% from community medical centers, representing diverse treatment settings. These treatment settings include academic, for-profit, community sites, and hospital systems in most of the US, with concentrations in the Northeast, Southeast, and South-Central regions of the US. Some examples of cancer centers include Miami Cancer Institute, Hackensack Meridian Health, John Theurer Cancer Center, Regional Cancer Care Associates, and Medstar Health.
COTA datasets contain individual patient data from the time of initial cancer diagnosis through to the most recent documentation in the EHR. Other available information includes patient demographics, cancer diagnosis, comorbidity, performance status, tumor histology, laboratory data, biomarker test methods and results, treatment information, and adverse events. All data available within the EHR at the time of abstraction were included in the RWE dataset. Where patients did not receive all of their care at a singular primary site, COTA reviewed and collected data from all available outside records that were scanned into the EHR and/or detailed by the treating physician. Patients who did not have sufficient documentation or had significant gaps in their patient journey within the EHR were excluded.
Compliance with Ethics Guidelines
All study data were fully compliant with US patient confidentiality requirements, including the Health Insurance Portability and Accountability Act (HIPAA) of 1996. The study used only de-identified patient records and, therefore, was exempted from institutional review board approval. Informed consent was not required, as this was not an interventional study, and routinely collected, anonymized data were used. This study complied with all relevant national regulations and was performed in accordance with the principles of the Declaration of Helsinki and the International Conference on Harmonization Guidelines on Good Clinical Practice. Full permission was received by COTA to access the study database.
Study Sample Selection
The study population included adult patients ≥ 18 years old with eNSCLC. A total of 1200 adult patients with a diagnosis of eNSCLC between January 1, 2000 and December 31, 2021 were initially identified by COTA, using the following patient identification and extraction criteria. Patients with a diagnosis of lung cancer were first identified based on having at least one international Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) code or ICD-10-CM code for lung cancer. Medical abstractors then manually confirmed the diagnosis in the EHR and completed the full patient record extraction. Patients with NSCLC were then identified based on the histology codes for NSCLC. eNSCLC patients were included in the study cohort based on having the disease at stage 0–IIIA. Patients were excluded if they met the following criteria: (1) they were < 18 years of age at the time of diagnosis; (2) they did not have the malignancy of interest (i.e., NSCLC); (3) they had no date of diagnosis in the EHR; (4) they had no clinician note available; (5) they were not evaluated at the accessible provider site for the malignancy of interest; or (6) they had concurrent primary malignancies. In our analyses, we further excluded patients who: (1) had a diagnosis of eNSCLC before 2011; (2) had an unspecified cancer stage; and (3) received biomarker testing prior to having a NSCLC diagnosis.
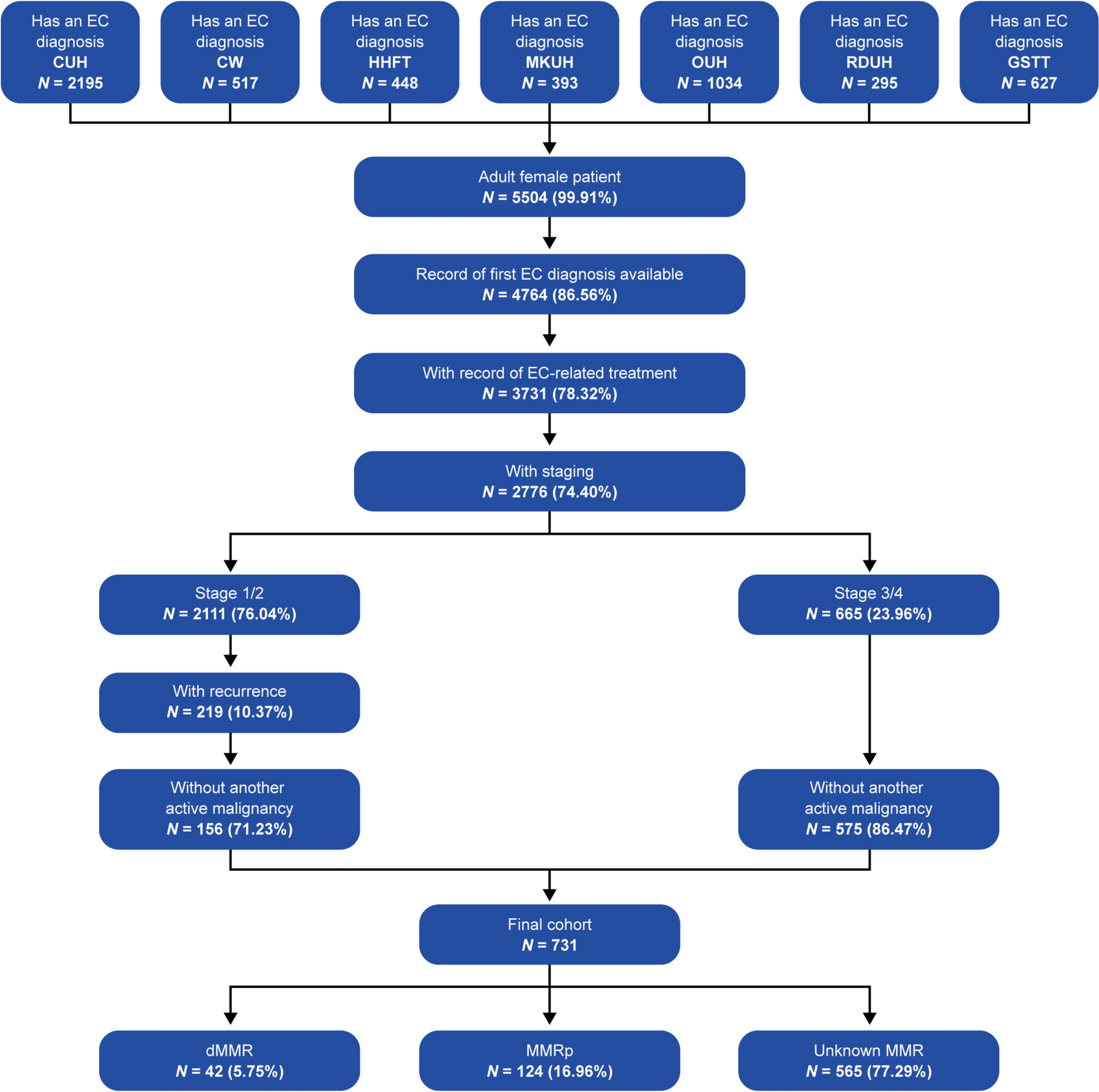
Additionally, for the study analysis, we limited the biomarker test utilization to within 6 months or 182 days of the eNSCLC diagnosis date. The 6-month cut-off date was specified because the study clinical expert advised that the majority of patients with eNSCLC are typically treated within 6 months of diagnosis. Patients were further required to have at least one medical activity, defined as having at least one office visit or treatment, within 182 days after eNSCLC diagnosis. To ensure that patients were actively receiving care within the COTA Health Database, patients were excluded if they had no evidence of an interaction with the healthcare system within 90 days of diagnosis or a survival of less than 30 days after the diagnosis date. Patients were also excluded if they enrolled in clinical trials within 182 days of eNSCLC diagnosis. A total of 1031 patients with eNSCLC were included in this analysis after applying these study eligibility criteria (Table 1).
Table 1 Attrition table: patient selection Three-month and 9-month cut-off dates were used for sensitivity analysis. Similar study sample sizes were found. The index date was the date of the first eNSCLC diagnosis. Patients were followed until death, the last medical activity date, or end of the study period, whichever occurred first.
Study Measures
Patients’ demographic and clinical characteristics were measured on or around the index date, including age at diagnosis, sex, race (e.g., white, African American, Asian, and other), ethnicity (Hispanic vs. non-Hispanic), cancer stage, Eastern Cooperative Oncology Group Performance Status Scale [21], personal history of cancer, history of tobacco usage, diagnosis method (i.e., biopsy, clinical, cytology, excisional biopsy, fine needle aspirate, surgical resection, other), and year of initial diagnosis.
The study database recorded details of the patients’ biomarker testing, such as the name of the molecular biomarker, test results (positive vs. negative), testing methods, specimen type, as well as dates of test collection and reporting. The specific testing methods included polymerase chain reaction, fluorescence in situ hybridization (FISH), immunohistochemistry (IHC), mutation-specific IHC, next-generation sequencing (NGS), ribonucleic acid (RNA) sequencing, Sanger sequencing, and unspecified. The specimen types included blood, tumor, and unspecified. The biomarker turnaround time was calculated as the difference between the date the specimen was collected in the laboratory and the date of the test result available to the provider.
Patients’ treatment information included surgery, radiation therapy, and systemic treatment regimens. We further categorized systemic treatment regimens into the following five categories: chemotherapies only, immunotherapies only, targeted therapies only, immunotherapy and chemotherapy (immuno-chemo), and targeted therapy and chemotherapy (targeted-chemo).
Statistical Analysis
Descriptive statistics were reported for the study, with the mean (median, minimum, maximum) used for continuous variables and the number (n) and proportion for categoric variables. The chi-squared test was used for categorical variables, and the t-test was performed for continuous variables to obtain p values.
To understand the biomarker test utilization over time, owing to the fact that biomarker testing rates were expected to change over the study time period between January 1, 2011 and December 31, 2021, we reported the biomarker testing rate by year of index diagnosis date for patients who received any biomarker test within 6 months of their eNSCLC diagnosis and by each molecular marker. We further evaluated the distribution of cancer stages, methods of testing, and specimen types among patients who received at least one biomarker test within 6 months of their eNSCLC diagnosis.
For treatment utilization, we reported the lines of therapy patients received within 1 year of their eNSCLC diagnosis. Additionally, in a subgroup of patients who received the five most commonly used biomarker tests, we reported the time from initial diagnosis to biomarker testing and the time from biomarker testing to first-line systemic treatment initiation. We further stratified our analysis by treatment type (i.e., chemotherapy vs. non-chemotherapy). All analyses were conducted using R version 4.2.0.

Comments (0)