
Remember me









Intra-articular distal radius fractures are frequently managed surgically with volar plating. A fracture pattern with separate scaphoid and lunate facets proposes an additional challenge in obtaining an adequate reduction of the articular surface. Typically, provisional fixation using kirschner wires (k wires) can be used to hold any separate fragments before definitive plate osteosynthesis. In the case of a sagittal intra-articular split, we have found that k-wire provisional fixation is inadequate in holding reduction of a comminuted joint surface (Figs. 1 and 2). Several intraoperative reduction maneuvers have been described, and anyone may be helpful depending on the specific deformity encountered.1–4 We propose a novel, plate-assisted reduction maneuver to more adequately reduce the articular surface.
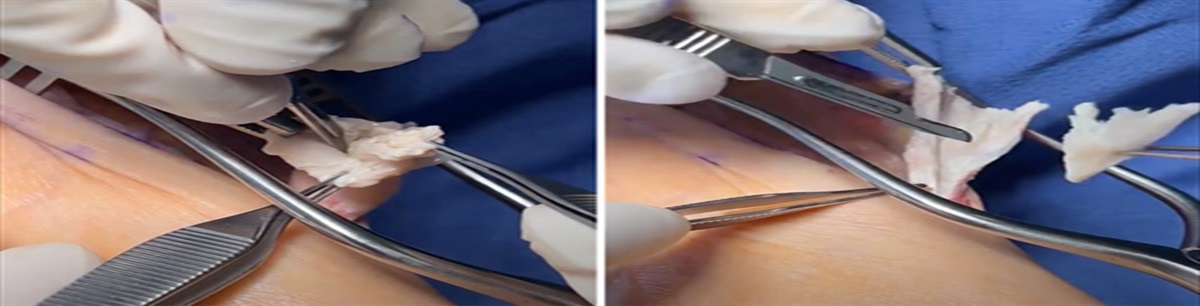
 FIGURE 1:
FIGURE 1: Provisional reduction of the radial styloid fragment to meta-diaphyseal segment using k-wire.
 FIGURE 2:
FIGURE 2: Construct following the removal of k-wire in the radial styloid fragment, revealing persistent intra-articular step-off.
TECHNIQUEThis maneuver is indicated in intra-articular distal radius fractures with a sagittal split creating separate scaphoid and lunate facet fragments. It can be used after failed provisional fixation of the articular surface with fragment-specific k-wire fixation. Materials needed for this maneuver include a volar distal radius plate with associated locking and cortical screws that are made for the plate of choice. Mini-c arm is the imaging of choice as it uses low-dose radiation and is typically easily maneuverable.
Figure 3 represents an intra-articular distal radius fracture with separate scaphoid and lunate facet fragments secondary to an intra-articular sagittal split. Following a standard trans-flexor carpi radialis volar approach to the distal radius, the radial artery is protected radially and the median nerve ulnarly with a blunt Hohmann retractor. The fracture is sharply debrided of hematoma, and cortices are visualized to help aid in reduction. Next, a reduction maneuver is used, with the initial exaggerated extension of the fracture, followed by dorsal pressure on the distal fragments with carpal translation. Mini-C images are used to ensure adequate restoration of the volar tilt of the distal radius at this time. A volar distal radius plate is then sized using fluoroscopic guidance. Next, the plate is provisionally fixed to bone in the center of the diaphyseal oblong hole to allow distalization of the plate in subsequent steps. Next, locking screws are placed into the radial scaphoid facet fragment to fully capture the distal radial fragment to the plate. Fluoroscopic guidance is then used to assess the amount of articular step-off that exists between the scaphoid facet and the ulnar lunate facet fragment. Next, the initial diaphyseal oblong hole screw is slightly loosened, and the plate is distalized under fluoroscopic guidance. Distalization of the plate can be achieved by using a freer or small cobb to push the plate distal as the initial cortical screw is briefly loosened. As the plate is distalized, the radial scaphoid facet fragment, captured by the locking screw fixation through the plate, is also distalized to align with the articular surface of the lunate facet. Once adequate reduction of the joint surface is achieved, the oblong hole screw is tightened back down to hold the reduction (Fig. 4). Finally, locking screw fixation can be placed to hold the ulnar lunate facet fragment to the plate, completing the construct (Fig. 5). After distalization of the plate and equal reduction of the articular surface, other components of the reduction can be addressed, such as gapping of the 2 fragments or inadequate volar tilt restoration.
 FIGURE 3:
FIGURE 3: Panel 1 demonstrates the initial fracture on presentation. Panel 2 is after reduction and splinting in the emergency room. Panel 3 is coronal CT demonstrating sagittal split, creating separate scaphoid and lunate facet fragments.
 FIGURE 4:
FIGURE 4: Construct after reduction maneuver, before locking screw fixation into ulnar lunate facet fragment.
 FIGURE 5:
FIGURE 5: Lateral x-ray demonstrating reduced articular surface.
The reverse deformity, a sagittal split leading to depression of the ulnar lunate facet, can be reduced in a similar fashion. A volar distal radius plate is fixed to bone in the center of the diaphyseal oblong hole. Next, locking screws are used to fix the plate to the depressed ulnar lunate facet. Next, the screw in the oblong hole is loosened, and the plate, which is fixed to the ulnar lunate facet, is distalized to achieve reduction to the articular radial surface. Once adequately reduced, the screw in the oblong hole is tightened to hold the reduction. Finally, locking screw fixation is filled into the radial scaphoid facet piece to complete the construct.
EXPECTED OUTCOMESThe expected outcome for this maneuver is an equivalent reduction of both the ulnar lunate facet and the radial scaphoid facet. This leads to an anatomically reduced joint line without accepting an intraoperative step-off of the ulnar lunate or radial scaphoid facet. We feel this technique provides a more stout and reliable maneuver to reduce these fragments than provisional k-wire fixation.
COMPLICATIONSThis technique is useful in achieving a more precise articular reduction of the distal radius. Some factors to consider include the initial plate placement as well as bone quality. If the plate is initially placed too distal, when the reduction maneuver is attempted, the plate may end too distal on the ulnar lunate facet fragment, which could cause symptomatic hardware at the joint line. In addition, caution should be used in very poor, osteoporotic bone when attempting this maneuver. As the plate is distalized, the locking screws in the radial scaphoid fragment are at risk of cutting out of osteoporotic bone as the relatively stronger plate-diaphyseal bone construct distalizes and “pushes” the articular segment towards more adequate reduction.
REFERENCES 1. Fox HM, Thompson AR, Nazir OF, et al. Use of a Large Tenaculum Clamp as a Reduction Technique for Treatment of Distal Radius Fractures. J Hand Surg Am. 2019;44:427.e1–427.e8. 2. Senehi R, Luo TD, Marquez-Lara A, et al. Use of Volar Plate for Indirect Coronal Plane Reduction in an Intraarticular Distal Radius Fracture. J Orthop Trauma. 2017;31(Suppl 3):S39–S41. 3. McLawhorn AS, Cody EA, Kitay A, et al. Leveraging the plate: reliably restoring volar tilt of distal radius fractures. Orthopedics. 2013;36:918–921. 4. Ross M, Allen L, Couzens GB. Correction of Residual Radial Translation of the Distal Fragment in Distal Radius Fracture Open Reduction. J Hand Surg Am. 2015;40:2465–2470.
Comments (0)