
Remember me
A 2-year-old female with a known case of congenital kyphosis was admitted to the hospital for scheduled correctional vertebroplasty, posterior spinal fusion, and spinal decompression at levels T12–L4. The patient was surgically free and developmentally mature for her age.
As part of the preoperative assessment, an MRI was done, which revealed a horseshoe kidney that her parents did not know of. Her preoperative labs were within a normal range (Table 1). The surgery went uneventfully, and a hip spica cast was applied. On post-operative assessment, the patient had normal neurological exam findings. After 2 days after surgery, she tolerated a regular diet, and the Foley catheter was removed.
Table 1 Laboratory tests. Laboratory tests showing the abnormal values after her vertebroplasty and the decrease after her exploratory laparotomyPost-operative day 4, the patient’s mother noticed that the patient developed fecal soiling; a digital rectal exam was performed, and deep rectal contractions were palpated; anal sphincter was not assessed as the patient was uncooperative. The next day, the patient vomited twice, two episodes of non-projectile vomiting consisting of partially digested food particles, which were associated with decreased oral intake. It was then followed by another episode of fecal vomiting. During the examination, the cast was found to be tight, putting pressure on her abdomen that protruded from the anterior window of the cast. The cast was split immediately, and we examined the abdomen; during palpation, the abdomen was slightly tense and distended, but no rigidity was noticed. Chest and abdominal X-rays were done, and no findings were seen. We inserted an NG tube and a Foley catheter and kept the patient on IV fluids and NPO; manual aspiration from the NG tube revealed 60 cc of fecal material.
The next day (post-op day 6), the patient was still experiencing episodes of vomiting despite the presence of an NG tube, and her abdomen was mildly distended and tender. She was tachycardic and febrile, and she passed small amounts of watery stool. She was transferred to the PICU for management and observation. Her labs showed evidence of acute kidney injury and dehydration, and her urine culture was positive for Escherichia coli.
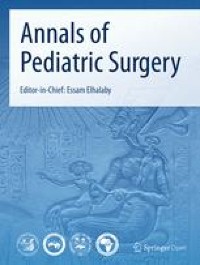
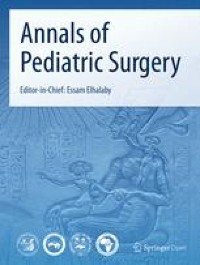
Meropenem (adjusted dose for her renal injury) and omeprazole were initiated. Chest and abdominal X-rays were repeated, and proximally dilated and distally collapsed bowels were noted (Fig. 1). The pediatric surgery team was consulted, and an impression of post-operative paralytic ileus was made. She was managed conservatively.
Fig. 1
Abdomen X-ray image showing proximally dilated small bowels and distally collapsed large bowels
The following day (post-op day 7), an abdomen and pelvis CT scan with contrast was ordered since there was no improvement in her status, and urine retention developed in the past 3 days. The CT scan showed dilated jejunal and mid-ileal loops with a narrow zone of transitions seen at the mid-ileal loops. Moderate free fluid was seen in the abdomen and pelvis. The findings were suggestive of mechanical obstruction, possibly adhesions.
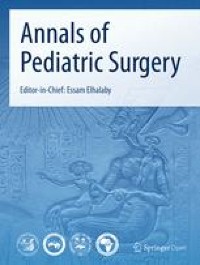
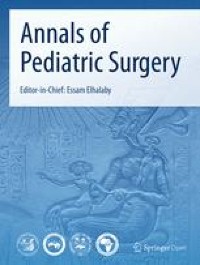
The pediatric surgery team mandated an urgent laparotomy. During the incision, a large amount of serous fluid gushed out the incision. Fibrous bands constricting the mid-ileal segment were released. Formal exploration of the stomach, liver, spleen, small bowels, large bowels, and retroperitoneum showed normal findings. Two perforations at the dome of the urinary bladder were found (Fig. 2); debridement of the necrotic tissue and refreshment of the edges were done first, then a primary double repair of the perforations with PDS 2–0 was done. A suprapubic catheter was inserted while keeping a urethral foley.
Fig. 2
An image was taken during surgery showing one of the perforations at the dome of the urinary bladder
The bladder was filled with normal saline to test the repair, and there was no leakage. After irrigation of the abdomen with saline, suctioning, and removal of all the fibrin co-material, another run of the bowel was done. All were healthy-looking.
The patient labs quickly normalized after the surgery; adequate urine output was noted, and she passed stool (Table 1). The NG tube was removed, and the patient tolerated oral intake on a clear fluid diet and then a regular diet with no vomiting. She was kept on IV omeprazole. The patient was discharged from the hospital 5 days after the laparotomy. A cystogram was done after 1 month, before removing the suprapubic catheter, and it showed no leakage of urine.
Comments (0)