
Remember me




Lichen sclerosus (LS) is a chronic inflammatory disease that predominantly affects the anogenital skin. Its etiology is unknown, although a strong association with autoimmune disease is recognized.1 An infectious etiology has also been suggested because LS has a genetic predisposition.2 The prevalence is estimated to range from 1:300 to 1:1,0003 and is even higher among elderly women.4 In general gynecological practice, the prevalence of vulvar LS is estimated at 1.7%5; however, the exact prevalence is difficult to ascertain because some patients remain asymptomatic. The diagnosis of LS is usually clinical.3
An association between vulvar squamous cell carcinoma (SCC) and vulvar LS is well documented. The lifetime risk of vulvar SCC in LS patients is estimated at 4% to 5%.6 A recent European study showed a cumulative incidence of vulvar SCC of 6.7% in LS patients after 20 years of follow-up.7 The reason for the malignant transformation from LS to SCC remains unknown. Lichen sclerosus has also been associated with a rare vulvar melanoma8 and basal cell carcinoma.9 In addition, some evidence supports an increased risk of vaginal cancer.10
Itching and soreness are common symptoms of LS. Postinflammatory scarring may cause alterations in the vulvar architecture, leading to dyspareunia and sexual dysfunction.11 Generally, LS has a significant impact on quality of life12,13 and has been linked to bladder, gastrointestinal, and pain comorbidities,14 but the research is still limited.
Some studies have suggested that certain vulvar diseases may represent symptoms of a generalized disorder of the pelvic floor as well as of other nearby structures, such as the bladder and bowel.15,16 Bladder and bowel disorders include overactive bladder (OAB), urinary incontinence, inflammatory bowel disease, constipation, and irritable bowel syndrome.14,17 Lichen sclerosus patients have been shown to have significantly more OAB, a greater prevalence of both stress and urgency incontinence, and a higher prevalence of irritable bowel syndrome.17 However, coexisting celiac disease has been reported in adults in only a case report of 1 LS patient.18
The aim of the present study was to evaluate the comorbidity of LS patients. We explored the risk of malignancies as well as the risks of urogynecological and gastrointestinal disorders. We hypothesized that not only are the risks of malignancies increased, but LS patients are also more likely to experience several benign urogynecological and gastrointestinal diseases and conditions.
METHODSThis cross-sectional case-control study included 455 women and girls with a diagnosis of LS who were treated for any reason at University Hospital from 2004 to 2012. Patients with a diagnosis of LS were identified by searching electronic medical records for International Classification of Diseases 10 (ICD-10) code L90.0. The diagnosis of LS was based on a clinical examination made by a specialist in gynecology. Among 455 LS patients, 259 patients had clinical diagnosis and 196 patients had histology-proven LS.
A 10-fold age- and sex-matched cohort with no diagnosis of LS served as a control cohort. This cohort was randomly selected from the University Hospital patient register. The health care district consists of more than 470,000 residents, and University Hospital serves as a tertiary clinic in 2 hospital districts.
The electronic patient register contains clinical data for all patients who visit public hospitals in the hospital district and includes administrative information, personal data, diagnosis, and diagnostic and treatment procedures. All diseases occurring in the cohorts during the study period were included. The diseases and conditions of interest were divided into: 1) cancers and their precursors (vulvar cancer, cervical cancer, endometrial cancer, ovarian cancer, breast cancer, vulvar high-grade squamous intraepithelial lesions [HSIL], differentiated-type vulvar intraepithelial neoplasia [dVIN], cervical squamous intraepithelial lesion [SIL]), 2) gynecological disorders (menorrhagia and postmenopausal bleeding [combined as menstrual disorders], inflammation of the vagina and vulva, anogenital condyloma, and/or vulvar low-grade squamous intraepithelial lesion [LSIL]), 3) pain syndromes (dyspareunia, interstitial cystitis), 4) urinary disorders (urinary incontinence), and 5) gastrointestinal disorders (diseases of the lip and oral mucosa, diverticular disease of the intestine, functional intestinal disorders, inflammatory bowel diseases like Crohn disease and ulcerative colitis, fissures of the anal and rectal regions, and celiac disease).
This study was approved by the clinical research center.
Statistical AnalysesWe compared the prevalence of diagnoses between LS patients and controls by calculating relative risks (RRs), confidence intervals (95% CIs), and p values for each diagnosis using the Pearson chi-square test. Patient age was calculated at the index date, which was chosen as the first occurrence of the LS diagnosis code in the electronic health records. All statistical tests were 2-tailed, and p < .05 was considered statistically significant. Statistical analysis was performed using R Statistics version 3.0.2 (Free Software Foundation, Boston, MA). Analysis of the patients with biopsy-proven LS was also conducted.
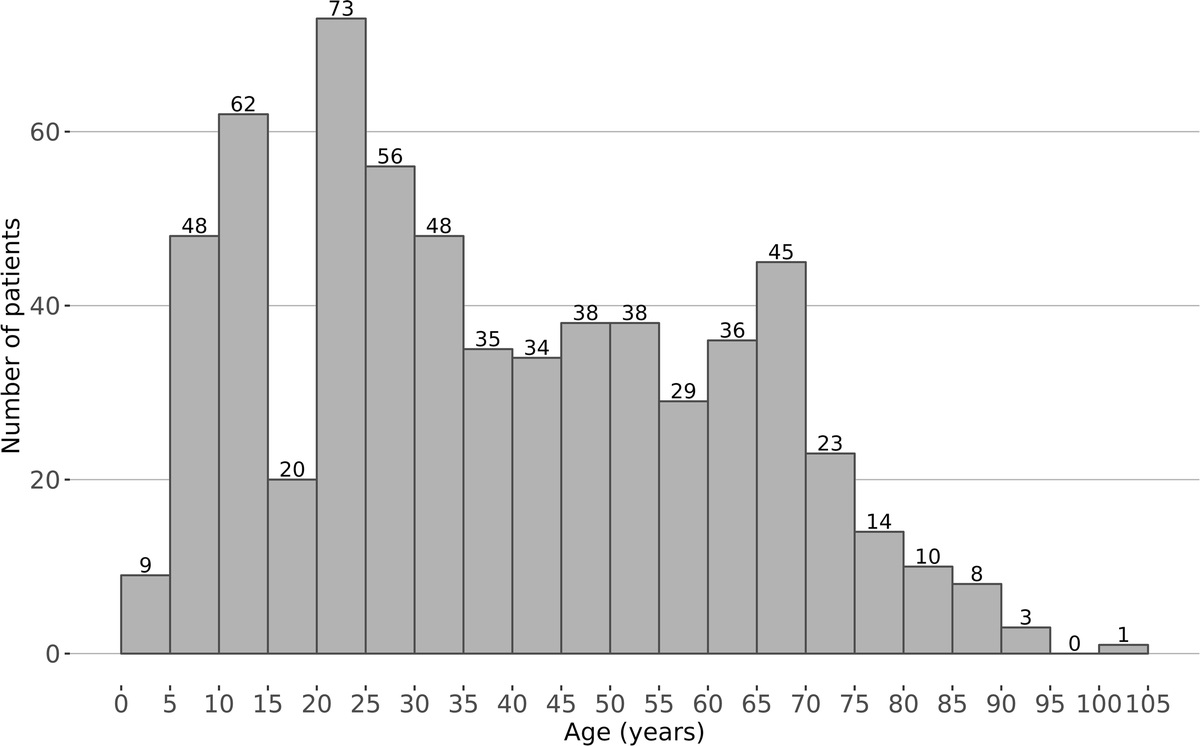
RESULTSA total of 455 women and girls with a diagnosis of LS were identified in the medical records registry. Overall, 93.4% of the LS patients and the controls lived in the hospital district. The mean age of the LS patients was 64 years (range = 6–104), and the age distribution is shown in Figure 1. The population of women and girls in the hospital district is approximately 250,000; thus, the prevalence of those referred for LS was 1.8:1,000 (95% CI = 1.6–2.0).
 FIGURE 1:
FIGURE 1: Age (years) distribution of 455 female patients with LS.
Gynecological Cancers and Precursors and LSWe found an increased risk for vulvar cancer in the LS patients compared with the control cohort (RR = 100.0; 95% CI = 50.9–196.4; p < .001). Twenty LS patients had a diagnosis of vulvar cancer, for a prevalence of 4.4%. Eighteen cases (90%) were histologically verified as SCC, and the other 2 were unspecified. Vulvar HSIL was increased in the LS patients (RR = 110.0; 95% CI = 14.2–850.1; p < .001). We also identified an additional 8 (1.8%) cases of vulvar dVIN in the LS patients, but none in the control cohort (Table 1).
TABLE 1 - Prevalence and Relative Risks of Gynecological Cancers and Precursors Found in 455 Women and Girls With LS and Their 4,550 Controls Gynecological cancers and precursors ICD-10 Prevalence in 455 women and girls with LS, % (n) Prevalence in 4,550 controls, % (n) RR 95% CI p Vulvar cancer C51 4.4 (20) 0.04 (2) 100.0 50.9–196.4 <0.001 Cervical cancer C53 0.7 (3) 0.1 (5) 6.0 1.7–21.1 0.005 Endometrial cancer C54 2.6 (12) 0.9 (41) 2.9 1.6–5.4 <0.001 Ovarian cancer C56 0.7 (3) 0.6 (26) 1.2 0.4–3.8 0.81 Breast cancer C50 4.6 (21) 4.3 (198) 1.1 0.7–1.7 0.79 Vulvar HSIL N90.1 N90.2 2.4 (11) 0.02% (1) 110.0 14.2–850.1 <0.001 Vulvar dVIN D07.1 1.8 (8) 0.0 (0) NA NA <0.001 Cervical SIL N87 1.5 (7) 0.7 (31) 2.3 1.0–5.0 0.044The risk of cervical cancer was higher (RR = 6.0; 95% CI = 1.7–21.1; p = .005) among LS patients, although only 3 cases were detected overall. The risk of cervical SIL was slightly higher in the LS patients than in the control cohort (RR = 2.3; 95% CI = 1.0–5.0; p = .044). One LS patient had vaginal SCC, but none in the control cohort did. The prevalence of endometrial cancer was also higher among the LS patients (RR = 2.9; 95%Cl = 1.6–5.4; p < .001). We did not find any associations with any other cancers. (Table 1).
Urogynecological Disorders, Pain Syndromes, and LSThe frequency of different gynecological disorders and uterine pathology, in addition to pain syndromes and urinary disorders, is shown in Table 2. Among the pain syndromes, dyspareunia and interstitial cystitis were diagnosed at higher rates in the LS patients than in the control cohort, even though the prevalences were quite low in both cohorts (1.3%). The RR was increased for dyspareunia (RR = 20.0; 95% CI = 7.5–53.1; p < .001) and interstitial cystitis (RR = 5.0; 95% CI = 2.1–12.1; p < .001). As for urinary disorders, we found that urinary incontinence was more common in the LS patients, with an RR of 4.8 (95% CI = 3.3–7.0; p < .001). Our evaluation of gynecological infections revealed an increased risk of vaginal and vulvar inflammation (RR = 13.1; 95% CI = 9.4–18.2; p < .001). Nine of our LS patients had ulcers in genital mucosa. Human papilloma virus (HPV)-related infections in the anogenital area were detected more often in the LS patients than in the control cohort (RR = 3.8; 95% CI = 2.1–6.7; p < .001). The risks of menorrhagia and postmenopausal bleeding (combined as menstrual disorders) were also elevated in the LS patients (RR = 2.5; 95% CI = 1.9–3.2; p < .001).
TABLE 2 - Prevalence and Relative Risks of Gynecological and Gastrointestinal Disorders Found in 455 Women and Girls With LS and Their 4,550 Controls Comorbidity ICD-10 Prevalence in 455 women and girls with LS, % (n) Prevalence in 4,550 controls, % (n) RR 95% CI p Gynecological disorders Menstrual disordersIn our study, oral lichen planus was found 10 times more often in LS patients. Oral symptoms were often nonspecific. Among gastrointestinal disorders, we found an increased risk of celiac disease in the LS patients (RR = 6.8; 95% CI = 3.7–12.5; p < .001) (Table 2). The risk for diverticular diseases of the intestine (RR = 1.9; 95% CI = 1.3–2.6; p < .001), functional intestinal disorders (RR = 2.3; 95% CI = 1.3–4.1; p = .003), and anal and rectal fissures was also increased in the LS patients (RR = 2.4; 95% CI = 1.0–5.7; p = .046), as was the risk of diseases of the lip and oral mucosa (RR = 4.8; 95% CI = 2.7–8.7; p < .001). The risk for inflammatory bowel diseases like Crohn disease or ulcerative colitis was not increased (RR = 1.3; 95% CI = 0.3–5.4; p = .77 for Crohn disease and RR = 0.7; 95% CI = 0.2–2.2; p = .54 for ulcerative colitis).
Findings in Patients With Biopsy-Proven LSOur subanalysis included the patients with LS confirmed by histological analysis, and the results are shown in Table 3. The findings were similar to those of the full analysis, but the association with cervical cancer was not confirmed.
TABLE 3 - Main Results of Gynecological and Gastrointestinal Disorders Found in 196 Patients With LS Confirmed by Biopsy and Their 10-Fold Age-Matched Cohort Comorbidity ICD-10 Prevalence in 196 women and girls with LS, % (n) Prevalence in 1,960 controls, % (n) RR 95% CI p Vulvar cancer C51 7.1 (14) 0.1 (2) 70.0 32.7–149.8 <0.001 Cervical cancer C53 0.5 (1) 0.1 (2) 5.0 0.6–43.3 0.14 Endometrial cancer C54 3.6 (7) 0.9 (17) 4.1 1.8–9.2 0.001 Vulvar HSIL and/or dVIN N90.1 N90.2 D07.1 3.6 (7) 0.0 (0) NA NA NA Celiac disease K90.0 2.0 (4) 0.3 (6) 6.7 2.2–19.9 0.001 Urinary incontinence N39.3 N39.4 R32 8.2 (16) 1.6 (31) 5.2 3.0–8.8 <0.001 Dyspareunia N94.1 1.5 (3) 0.1 (1) 30.0 7.0–128.3 <0.001 Interstitial cystitis N30.1 2.0 (4) 0.3 (6) 6.7 2.2–19.9 0.001We verified the previously reported association between LS and vulvar cancer, while also identifying the novel finding of increased risk for other gynecological cancers (e.g., cervical and endometrial cancer). Lichen sclerosus patients were also more likely to experience different benign urogynecological disorders, including inflammation of the vulva and vagina, menorrhagia, and urinary incontinence, as well as pain syndromes like dyspareunia and interstitial cystitis. Lichen sclerosus patients also had a higher risk of gastrointestinal disorders, including celiac disease, diverticular intestinal diseases, functional intestinal disorders, and anal and rectal fissures, suggesting significant comorbidity in LS. Some associations were probably consequences of LS or immunosuppressive LS treatments, but common pathophysiologic pathways are plausible.
Lichen sclerosus patients had increased risk of vulvar cancer, mostly SCCs, as reported previously,6–8 but different vulvar malignancies have been reported with LS.9 Vulvar SCC may arise by HPV-associated pathway via vulvar HSIL or by HPV-independent pathway via LS-associated dVIN. Progression of dVIN to vulvar SCC is frequently missed,19 and the low number of LS patients with SIL diagnosed with dVIN may result from misclassification.7 We did not reevaluate the histopathological features of diagnoses of vulvar SIL; however, SIL changes were frequently found, suggesting a need for biopsy and meticulous follow-up in women with LS and any type of SIL.
We also found a slightly increased risk of cervical cancer and cervical SIL in our LS patients. In our country, cervical cancer is a rare disease, with an annual incidence of 6.1/100,000 women (www.cancerregistry.fi), and we identified 3 patients with both cervical cancer and LS. Human papillomavirus is the main risk factor for cervical cancer, and our LS patients showed increases in HPV-related infections in the anogenital area. Immunosuppressive medications, such as topical steroids used in the treatment for LS, could be one explanation, although another could be the existence of an underlying immunodeficiency in LS that allows HPV to thrive. However, we could not totally exclude the fact that the LS patients had more visits rather than the control group, maximizing the probability to evidence HPV-related infections. Nevertheless, HPV infections have been shown to have a role in the development of LS.20 Patients with vulvar cancer related to HSIL have an increased incidence of cervical malignancies due to high-risk HPV.21 However, previous cervical HSIL is also a risk factor for both cervical and vulvar cancer, even though only 15% to 17% of invasive vulvar cancer cases in elderly women are associated with high-risk HPV infections.22,23 Human papillomavirus might also have an etiopathogenic role in anogenital LS, but the association is unclear.20
Our LS patients had an increased risk of endometrial cancer, an association that has not been reported previously. Accordingly, the pathogenesis and development of LS may not be solely dermatologic, but may also be associated with metabolic and lifestyle factors. Hypertension, type 2 diabetes, and overweight are more common among the patients with LS,24,25 but older age, obesity, and diabetes are also risk factors for endometrial cancer and could explain the increased risk in LS patients. Menorrhagia and postmenopausal bleeding were combined because patients with different types of bleeding usually have to use sanitary towels for long periods, and the moist sanitary towels may cause irritation in vulvar mucosa. This could at least partly explain the association between menstrual disorders and LS.
Our findings were in discrepancy with a large register-based study, where the risk of cervical and endometrial cancers was not elevated in LS patients.10 The reason for this discrepancy is the difference in study methods: our study was a cross-sectional study, where the cancer might also have preceded the LS diagnosis. The study of Halonen et al.10 was a register-based study, where they evaluated the incidence of the cancer diagnosis after LS diagnosis.
Infections of the vagina and vulva were also more common in the LS patients and were mainly chronic. It is possible that in inexperienced hands, LS patients might be misdiagnosed as having, for example, vulvitis. Lichen sclerosus presumably alters the regulation of the inflammatory system by an infectious etiologic of LS, as the disease itself, or as a consequence of LS treatment. In our study, 9 of our LS patients had ulcers in genital mucosa, although it is very rarely seen in LS. Our LS patients also showed a higher prevalence of dyspareunia, and chronic infection could especially contribute to this symptom. Hence, LS may cause sexual dysfunction.11 Actually, women with LS reportedly have less frequent sexual activity and are less satisfied with sexual life.11 Vulvar pain and symptoms, for any reason, may affect mental and physical health crucial for sexual health.26
In agreement with previous studies,17,27 lower urinary tract symptoms were more common in our LS patients. Similar rates of lower urinary tract symptoms have been described in women with biopsy-proven LS and vulvar diseases without LS.17 In our study, the risk for interstitial cystitis was 5 times greater in the LS patients than in the control cohort, and the LS patients also experienced more urinary incontinence (stress and urgency incontinence). Chronic irritation from exposure to liquids, such as urine, may be the triggering factor.3 In general, OAB seems to be the most predominant type of lower urinary tract LS symptom.27 Women with LS have been reported to have a higher prevalence of both OAB and urinary incontinence,17 but OAB was not more frequent in our LS patients. In our country, OAB symptoms without incontinence are predominantly diagnosed and treated in primary health care or private clinics. The diagnoses in the present study were collected only from our tertiary referral clinic and possibly reflected patients with more severe symptoms, which could have led to bias concerning the occurrence of OAB.
Previous studies have shown an association between LS and bowel comorbidities.14 In our study of gastrointestinal disorders associated with LS, the risk of celiac disease was notable. However, the risk for Crohn disease or ulcerative colitis in LS patients was not increased. An autoimmune association with vulvar LS has been demonstrated previously in many studies.1,28 However, a co-occurrence of celiac disease in LS has not been widely reported. One published study has shown a co-occurrence in pediatric patients with LS,13 whereas another is a case report of celiac disease in 1 woman with LS.18 Thus, celiac disease should be considered among other autoimmune diseases during follow-up of LS patients.
In agreement with previous studies, the risk of functional bowel disorders, such as constipation and diarrhea, was increased among the LS patients. We also found a greater prevalence of diverticular disease of the intestine among our LS patients, likely a reflected consequence of constipation. In our study, the LS patients also had more anal fissuring and nonspecific gastrointestinal bleeding. These may represent manifestations of LS rather than being separate entities. Estimates of the frequency of gastrointestinal disorders vary widely,14,17 but constipation is a common symptom in pediatric LS patients. In children with LS, 89% have at least 1 gastrointestinal-related complaint (bleeding with bowel movements, fissuring, soiling fecal impaction, or constipation).29
Our study had some limitations. Because in our study design, the diagnosis of LS was clinical, based on the guidelines of the European Dermatology Forum,3 some patients with negative histology could be also included in the study. Another limitation was that the data were collected from medical records, and the diagnosis was included only if it was entered with an ICD code. For example, ICD-10 code D07.1 certainly contains only dVIN diagnosis, but code N90.2 might include both vulvar HSIL and dVIN. Thus, we have no information regarding cases with diagnoses recorded as free text in the medical records, although the diagnosis of LS in our study was defined by a specialist in gynecology. We were unable to gather information on known confounders, including parity, body mass index, and smoking habits, which may have accounted for our findings. The present findings were based on prevalent LS cases with no follow-up data. The cross-sectional study design precluded determination of whether the comorbidities were diagnosed before or after the LS diagnosis. In the current analysis, the prevalence of LS was 1.8:1,000, in line with prevalence estimations in other publications.4,30 Thus, we assume that our dataset is a representative sample of LS in women and girls. Our results were verified in patients with biopsy-proven LS, which strengthens the study.
CONCLUSIONSOur results indicate that LS patients are at risk for several comorbidities. Some of these may act as triggers for the development of LS, whereas others are clearly LS consequences, suggesting a complex pathophysiology for LS. Thus, LS-associated comorbidities may also have a significant effect on quality of life and should be considered when treating patients with LS.
REFERENCES 1. Cooper SM, Ali I, Baldo M, et al. The association of lichen sclerosus and erosive lichen planus of the vulva with autoimmune disease: a case-control study. Arch Dermatol 2008;144:1432–5. 2. Sherman V, McPherson T, Baldo M, et al. The high rate of familial lichen sclerosus suggests a genetic contribution: an observational cohort study. J Eur Acad Dermatol Venereol 2010;24:1031–4. 3. Kirtschig G, Becker K, Günthert A, et al. Evidence-based (S3) guideline on (anogenital) lichen sclerosus. J Eur Acad Dermatol Venereol 2015;29:e1–43. 4. Leibovitz A, Kaplun V, Saposhnicov N, et al. Vulvovaginal examinations in elderly nursing home women residents. Arch Gerontol Geriatr 2000;31:1–4. 5. Goldstein AT, Marinoff SC, Christopher K, et al. Prevalence of vulvar lichen sclerosus in a general gynecology practice. J Reprod Med 2005;50:477–80. 6. van de Nieuwenhof HP, van der Avoort IAM, de Hullu JA. Review of squamous premalignant vulvar lesions. Crit Rev Oncol Hematol 2008;68:131–56. 7. Bleeker MCG, Visser PJ, Overbeek LIH, et al. Lichen sclerosus: incidence and risk of vulvar squamous cell carcinoma. Cancer Epidemiol Biomarkers Prev 2016;25:1224–30. 8. Hieta N, Kurki S, Rintala M, et al. Association of vulvar melanoma with lichen sclerosus. Acta Derm Venereol 2019;99:339–40. 9. Comstock JR, Woodruff CM, Yu SS, et al. Vulvar basal cell carcinoma in a patient with long-standing lichen sclerosus. JAAD Case Rep 2019;5:69–71. 10. Halonen P, Jakobsson M, Heikinheimo O, et al. Lichen sclerosus and risk of cancer. Int J Cancer 2017;140:1998–2002. 11. Haefner HK, Aldrich NZ, Dalton VK, et al. The impact of vulvar lichen sclerosus on sexual dysfunction. J Womens Health (Larchmt) 2014;23:765–70. 12. Lansdorp CA, Van Den Hondel KE, Korfage IJ, et al. Quality of life in Dutch women with lichen sclerosus. Br J Dermatol 2013;168:787–93. 13. Lagerstedt M, Karvinen K, Joki-Erkkilä M, et al. Childhood lichen sclerosus—a challenge for clinicians. Pediatr Dermatol 2013;30:444–50. 14. Berger MB, Damico NJ, Menees SB, et al. Rates of self-reported urinary, gastrointestinal, and pain comorbidities in women with vulvar lichen sclerosus. J Low Genit Tract Dis 2012;16:285–9. 15. Kennedy CM, Nygaard IE, Saftlas A, et al. Vulvar disease: a pelvic floor pain disorder?Am J Obstet Gynecol 2005;192:1829–35. 16. Kennedy CM, Nygaard IE, Bradley CS, et al. Bladder and bowel symptoms among women with vulvar disease: are they universal?J Reprod Med 2007;52:1073–8. 17. Swenson CW, Menees SB, Haefner HK, et al. Lower urinary tract and functional bowel symptoms in women with vulvar diseases and controls. Female Pelvic Med Reconstr Surg 2015;21:211–4. 18. Karadag AS, Kavala M, Ozlu E, et al. The co-occurrence of lichen sclerosus et atrophicus and celiac disease. Indian Dermatol Online J 2014;5:S106–8. 19. van de Nieuwenhof HP, Bulten J, Hollema H, et al. Differentiated vulvar intraepithelial neoplasia is often found in lesions, previously diagnosed as lichen sclerosus, which have progressed to vulvar squamous cell carcinoma. Mod Pathol 2011;24:297–305. 20. Hald AK, Blaakaer J. The possible role of human papillomavirus infection in the development of lichen sclerosus. Int J Dermatol 2018;57:139–46. 21. de Bie RP, van de Nieuwenhof HP, Bekkers RLM, et al. Patients with usual vulvar intraepithelial neoplasia-related vulvar cancer have an increased risk of cervical abnormalities. Br J Cancer 2009;101:27–31. 22. de Sanjosé S, Alemany L, Ordi J, et al. Worldwide human papillomavirus genotype attribution in over 2000 cases of intraepithelial and invasive lesions of the vulva. Eur J Cancer 2013;49:3450–61. 23. Coffey K, Gaitskell K, Beral V, et al. Past cervical intraepithelial neoplasia grade 3, obesity, and earlier menopause are associated with an increased risk of vulval cancer in postmenopausal women. Br J Cancer 2016;115:599–606. 24. Virgili A, Borghi A, Cazzaniga S, et al. New insights into potential risk factors and associations in genital lichen sclerosus: data from a multicentre Italian study on 729 consecutive cases. J Eur Acad Dermatol Venereol 2017;31:699–704. 25. Hieta N, Rintala M, Söderlund JM, et al. Comorbidity of dermal and cardiovascular disorders with lichen sclerosus: a case-control study. Acta Derm Venereol 2021;101:adv00594. 26. Sargeant HA, O’Callaghan FV. The impact of chronic vulval pain on quality of life and psychosocial well-being. Aust N Z J Obstet Gynaecol 2007;47:235–9. 27. Christmann-Schmid C, Hediger M, Gröger S, et al. Vulvar lichen sclerosus in women is associated with lower urinary tract symptoms. Int Urogynecol J 2018;29:217–21. 28. Kreuter A, Kryvosheyeva Y, Terras S, et al. Association of autoimmune diseases with lichen sclerosus in 532 male and female patients. Acta Derm Venereol 2013;93:238–41. 29. Maronn ML, Esterly NB. Constipation as a feature of anogenital lichen sclerosus in children. Pediatrics 2005;115:e230–2. 30. Preti M, Joura E, Vieira-Baptista P, et al. The European Society of Gynaecological Oncology (ESGO), the International Society for the Study of Vulvovaginal Disease (ISSVD), the European College for the Study of Vulval Disease (ECSVD) and the European Federation for Colposcopy (EFC) consensus statements on pre-invasive vulvar lesions. J Low Genit Tract Dis 2022;26:229–44.
Comments (0)