

Remember me








When caring for heart failure patients during the pandemic, all indirect and direct factors should be considered.
The coronavirus disease 2019 (COVID-19) pandemic, caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has significantly impacted the public health on a global scale. It was first reported in Wuhan, China, in December 20191Holshue ML DeBolt C Lindquist S et al.First Case of 2019 Novel Coronavirus in the United States. and has since spread globally, infecting over 651 million people and causing over 6.65 million deaths as of December 2022. While the most well-known complication of COVID-19 is respiratory failure, the infection can also lead to dysfunction in multiple organ systems, including the cardiovascular system. This can range from mild myocardial injury to more severe conditions such as myocardial infarction, heart failure (HF), and cardiogenic shock, potentially leading to cardiovascular death. 3Clerkin KJ Fried JA Raikhelkar J et al.COVID-19 and Cardiovascular Disease., 4Zheng YY Ma YT Zhang JY Xie X COVID-19 and the cardiovascular system., 5Madjid M Safavi-Naeini P Solomon SD Vardeny O Potential Effects of Coronaviruses on the Cardiovascular System.This review will explore the impacts of COVID-19 on individuals with pre-existing HF, the incidence and risk factors for subsequent HF in COVID-19 patients, the relationship between COVID-19 and cardiogenic shock, and the indirect impacts of COVID-19 on HF care.
COVID-19 and Pre-Existing HFHF is a common pre-existing condition among COVID-19 patients and can lead to poor prognoses. Studies found that between 4.9% and 13% of hospitalized COVID-19 patients also had HF.9Petrilli CM, Jones SA, Yang J, et al. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ. 2020;369:m1966. doi:10.1136/bmj.m1966
, 10Lala A Johnson KW Januzzi JL et al.Prevalence and Impact of Myocardial Injury in Patients Hospitalized With COVID-19 Infection., 11Richardson S Hirsch JS Narasimhan M et al.Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area., 12Rey JR Caro‐Codón J Rosillo SO et al.Heart failure in COVID‐19 patients: prevalence, incidence and prognostic implications., 13Alvarez-Garcia J Lee S Gupta A et al.Prognostic Impact of Prior Heart Failure in Patients Hospitalized With COVID-19., 14Goyal P Reshetnyak E Khan S et al.Clinical Characteristics and Outcomes of Adults With a History of Heart Failure Hospitalized for COVID-19. These patients tended to have higher levels of certain biomarkers, such as troponin and BNP and were at increased risk of needing mechanical ventilation and having a longer stay in the intensive care unit.12Rey JR Caro‐Codón J Rosillo SO et al.Heart failure in COVID‐19 patients: prevalence, incidence and prognostic implications.,13Alvarez-Garcia J Lee S Gupta A et al.Prognostic Impact of Prior Heart Failure in Patients Hospitalized With COVID-19. In addition, the risk of in-hospital mortality increased in COVID-19 patients with concomitant HF compared to those without the condition after adjusted for confounders (Figure 2).13Alvarez-Garcia J Lee S Gupta A et al.Prognostic Impact of Prior Heart Failure in Patients Hospitalized With COVID-19.,14Goyal P Reshetnyak E Khan S et al.Clinical Characteristics and Outcomes of Adults With a History of Heart Failure Hospitalized for COVID-19.Figure 2Pre-existing HF is an independent risk factor for intensive care unit stay, intubation, and in-hospital mortality after adjusted for confounding factors in patients with COVID-19 infection.
Show full captionAdapted from Alvarez-Garcia J, Lee S, Gupta A, et al. Prognostic Impact of Prior Heart Failure in Patients Hospitalized With COVID-19. J Am Coll Cardiol. 2020;76(20):2334-2348.
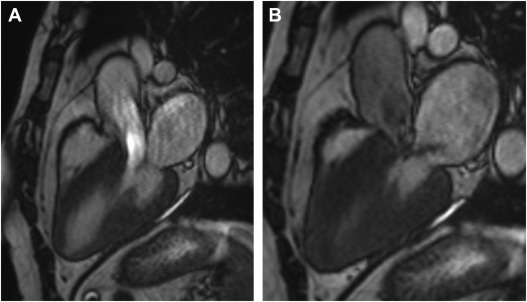
There was also initial concern about the potential effects of certain medications, used to treat HF, on the risk of SARS CoV-2 infection, such as angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin II receptor blockers (ARBs).15COVID-19 and Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers. Some pre-clinical data suggested that ACEIs and ARBs might upregulate ACE2 receptors, which increases the risk of SARS-CoV-2 infection. As a result, there was a shift towards using fewer ARBs or ACEIs for these conditions. However, multiple subsequent studies found no relationship between the use of ACEIs or ARBs and the severity of COVID-19 infection, and a meta-analysis of 11 randomized controlled trials suggested no difference in the risk of all-cause mortality.16Gnanenthiran SR Borghi C Burger D et al.Renin‐Angiotensin System Inhibitors in Patients With COVID‐19: A Meta‐Analysis of Randomized Controlled Trials Led by the International Society of Hypertension. Overall, despite longer length of stay and higher short-term mortality in patients with HF and concomitant COVID-19 infection, adherence to heart failure quality measures such as sustained to minimally increased prescription of guideline-directed medical therapies was largely maintained during the pandemic.17Keshvani N Mehta A Alger HM et al.Heart failure quality of care and in-hospital outcomes during the COVID-19 pandemic: findings from the Get With The Guidelines-Heart Failure registry. In terms of withdrawing from guideline-directed medical therapy (GDMT) and mortality rates, discontinuing the GDMT medications prescribed during hospitalization was significantly associated with an increased risk of in-hospital mortality.12Rey JR Caro‐Codón J Rosillo SO et al.Heart failure in COVID‐19 patients: prevalence, incidence and prognostic implications.However, overall HF care has been impacted by the pandemic in various ways. There is evidence that the number of acute HF hospitalizations decreased significantly during the pandemic, with a 27% reduction in daily admissions observed in a large German study during the early months of the pandemic compared to the previous year.17Keshvani N Mehta A Alger HM et al.Heart failure quality of care and in-hospital outcomes during the COVID-19 pandemic: findings from the Get With The Guidelines-Heart Failure registry. This decrease was felt to be related to the implementation of social distancing measures, increased use of telemedicine, and changes in healthcare seeking behavior.17Keshvani N Mehta A Alger HM et al.Heart failure quality of care and in-hospital outcomes during the COVID-19 pandemic: findings from the Get With The Guidelines-Heart Failure registry.COVID-19 and new-onset HFThere are several potential mechanisms to account for the cardio-toxic effects of SARS-CoV-2, including direct viral and immune-mediated damage, leading to inflammation with subsequent myocardial injury, edema, and myocarditis; demand ischemia due to respiratory failure and hypoxemia; and post-viral autoimmune reactions.18Kawakami R Sakamoto A Kawai K et al.Pathological Evidence for SARS-CoV-2 as a Cause of Myocarditis. Possible factors that may worsen HF in patients with COVID-19 include increased oxygen demand, myocarditis, stress-induced cardiomyopathy, ischemia, increased pulmonary pressure, and venous thromboembolism.19DeFilippis EM Reza N Donald E Givertz MM Lindenfeld J Jessup M Considerations for Heart Failure Care During the COVID-19 Pandemic.COVID-19 has been implicated in vascular endothelial damage. Systemic inflammation caused by SARS-CoV-2 leads to significant platelet activation. The increased levels of pro-inflammatory interleukins on the surface receptors of platelets as well as the reduction of endothelial nitric oxide are what causes this phenomenon. Simultaneously, neutrophils expression adhesion molecules supporting platelet aggregation. These mechanisms, along with endothelial damage, lead to aggravation of the thrombo-inflammatory pathway of COVID-19.20Theofilis P Sagris M Antonopoulos AS Oikonomou E Tsioufis C Tousoulis D Inflammatory Mediators of Platelet Activation: Focus on Atherosclerosis and COVID-19. Hence, COVID-19 has led to abnormal activation of immune responses during infection, leading to suboptimal myocardial repair with increased incidence of HF.21Inflammation and resolution signaling in cardiac repair and heart failure. MI have been shown to increase the incidence of HF, a study of patient over the age of 65 showed that 76% of patient who survived their first acute myocardial infarction developed HF in the next 5 years.22Ezekowitz JA Kaul P Bakal JA Armstrong PW Welsh RC McAlister FA Declining In-Hospital Mortality and Increasing Heart Failure Incidence in Elderly Patients With First Myocardial Infarction.Another potential mechanism of COVID-19-induced HF include endothelial injury coupled with micro-thrombi which could damage the endocardium. Several reports showed that the endothelium of organs contains ACE2 receptors and invasion receptors by SARS-CoV-2 resulting in an immediate inflammatory response with activation of the complement and thrombin system. All of these pathophysiological reactions lead to the development of coagulopathy with elevated D-dimer and fibrin products, leading to subsequent development of micro-thrombi.23COVID–19-associated coagulopathy: An exploration of mechanisms.,24McFadyen JD Stevens H Peter K The Emerging Threat of (Micro)Thrombosis in COVID-19 and Its Therapeutic Implications. In patients who died from COVID-19, inflammation of the capillaries with micro-thrombi were observed in the early disease course. Large thrombi, microangiopathy, and signs of disseminated intravascular coagulation were observed in the more chronic and serious cases of COVID-19.25Bösmüller H Traxler S Bitzer M et al.The evolution of pulmonary pathology in fatal COVID-19 disease: an autopsy study with clinical correlation. This coagulopathy and micro thrombosis dysfunction of vascular endothelium in COVID-19 patients is associated with development of myocardial injury and HF. Other studies show that endothelial injury may lead to increased vascular permeability and low nitric oxide level in the internal layer of the capillary.26COVID-19, Renin-Angiotensin System and Endothelial Dysfunction. All of these components could lead to severe cardiac injury causing HF.Early cases of COVID-19 in the United States revealed that cardiomyopathy developed in a significant proportion of patients. However, it is unclear whether the high rates of cardiomyopathy were a direct cardiac complication from SARS-CoV-2 infection or a result of critical illness.27Arentz M Yim E Klaff L et al.Characteristics and Outcomes of 21 Critically Ill Patients With COVID-19 in Washington State. Pathogenesis of COVID-19 cardiomyopathy is related to previously described inflammatory cytokines, leading to diastolic dysfunction and increased myocardial wall stiffness facilitated by IL-6 and myocardial fibrosis induced by IL-1β and tumor necrosis factor α.28Song Y Gao P Ran T et al.High Inflammatory Burden: A Potential Cause of Myocardial Injury in Critically Ill Patients With COVID-19. In Wuhan, of 191 hospitalized patients, HF was found in half of the fatal cases and in 12% of survivors.29Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. These observations were later confirmed in a second Chinese study of 799 COVID-19 hospitalized patients. In addition, 49% of 113 deceased patents with COVID-19 had complications of acute HF during their clinical course.30Chen T Wu D Chen H et al.Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study. Furthermore, elevated NT-pro-BNP at the time of admission for COVID-19 hospitalization was associated with an increased risk of inpatient mortality. NT-pro-BNP elevations independently predicted a 2 to 7 times increased rate of mortality based on a large nationwide cohort.31O’Donnell C Ashland MD Vasti EC et al.N‐Terminal Pro‐B‐Type Natriuretic Peptide as a Biomarker for the Severity and Outcomes With COVID‐19 in a Nationwide Hospitalized Cohort. Hospital mortality rates in patients with acute HF and COVID-19 were extremely high, up to 44% at the height of the pandemic.After the acute phase, COVID-19 may be responsible for HF as a long-term cardiovascular complication, but further clinical studies are needed.6Italia L Tomasoni D Bisegna S et al.COVID-19 and Heart Failure: From Epidemiology During the Pandemic to Myocardial Injury, Myocarditis, and Heart Failure Sequelae. In a study, they observed more than 3000 patients with confirmed COVID-19 infections and followed them for 30 days. They found that 77 patients, about 2.5%, developed symptoms of acute HF during this study period. Echocardiographic examinations were available for 31 patients with some degree of left ventricular systolic dysfunction. Seventeen patients had other findings, such as valvular heart disease, pericardial effusion, or right ventricular dysfunction.12Rey JR Caro‐Codón J Rosillo SO et al.Heart failure in COVID‐19 patients: prevalence, incidence and prognostic implications. Echocardiography performed within the first 24 hours in 100 COVID-19 patients showed predominantly an initial deterioration of right ventricular function by dilation and dysfunction, followed by the development of left ventricular dysfunction, and worsening LV systolic dysfunction in 10% of patients.32Szekely Y Lichter Y Taieb P et al.Spectrum of Cardiac Manifestations in COVID-19. Right ventricular dysfunction was present in large proportions of hospitalized patients with predictive value for poor outcomes.33Bieber S Kraechan A Hellmuth JC et al.Left and right ventricular dysfunction in patients with COVID-19-associated myocardial injury. ICU level patients with severe COVID-19 requiring persistent ventilation can lead to increased RV afterload from elevated positive pressures, thus inducing additional strain in the ventricle and further reducing the already impaired cardiac output.34Miftode RS Petriș AO Onofrei Aursulesei V et al.The Novel Perspectives Opened by ST2 in the Pandemic: A Review of Its Role in the Diagnosis and Prognosis of Patients with Heart Failure and COVID-19.Viruses are known to stimulate a cell-mediated immune response, which causes myocarditis and may progress to dilated cardiomyopathy.35Inflammation in myocardial disease: From myocarditis to dilated cardiomyopathy. Previous case reports of myocarditis in COVID-19 patients provided evidence of cardiac inflammation, with inflammatory infiltrates leading to regions of cardiomyocyte necrosis leading to myocarditis.36Yao XH Li TY He ZC et al.[A pathological report of three COVID-19 cases by minimal invasive autopsies]. Proposed mechanisms include specific infectious causes that alter the myocyte membrane, which trigger an immune response, which consists of predominate macrophage and lymphocyte infiltration of myocardial tissue. A large recent review of postmortem histopathologic data showed a high prevalence of myocardial necrosis and edema without myocarditis, due to a lack of inflammatory infiltrates. This may be related to the microthrombi described earlier.37Almamlouk R Kashour T Obeidat S et al.COVID-19–Associated cardiac pathology at the postmortem evaluation: a collaborative systematic review. In most patients, after the initial viral infection, the immune response clears the pathogen, and usually the inflammation resolves. However, for a group of patients with altered immune reactivity, they can develop an autoimmune reactivation leading to acute myocardial disease and cardiac dysfunction.38Tymińska A Ozierański K Caforio ALP et al.Myocarditis and inflammatory cardiomyopathy in 2021 – an update. The incidence of COVID-19 myocarditis is uncertain. A recent systemic review revealed that the prevalence of definite acute myocarditis among hospitalized patients with COVID-19 was 2.4 per 1000 hospitalizations, and that number was increased to 4.1 per 1000 to include possible acute myocarditis.39Ammirati E Lupi L Palazzini M et al.Prevalence, Characteristics, and Outcomes of COVID-19–Associated Acute Myocarditis. In a study of 100 patients who had recovered from severe COVID-19 infection, it was found that 78% of them had an evidence of cardiac involvement as seen on cardiac MRI, and 60% of them had ongoing myocardial inflammation, regardless of preexisting conditions, severity and course of their acute illness. MRI injury patterns and included a raised myocardial native T2, non-ischemic myocardial LGE, pericardial enhancement, and an ischemic pattern LGE.40Puntmann VO Carerj ML Wieters I et al.Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered From Coronavirus Disease 2019 (COVID-19).Stress-induced cardiomyopathy with apical ballooning was also documented in patients with COVID-19. In a case report, a patient with COVID-19 without a history of cardiovascular diseases developed and received from clinical stress cardiomyopathy.41Tsao CW Strom JB Chang JD Manning WJ COVID-19–Associated Stress (Takotsubo) Cardiomyopathy. A retrospective cohort study, found a significant incidence of stress induced cardiomyopathy during the COVID-19 pandemic compared with pre-pandemic periods. Of note, all of these patients tested negative for COVID-19 during the pandemic period. The psychological, social and economic distress accompanying the pandemic likely led to an increased risk of stress induced cardiomyopathy, rather than direct viral involvement.42Jabri A Kalra A Kumar A et al.Incidence of Stress Cardiomyopathy During the Coronavirus Disease 2019 Pandemic. Stress-induced cardiomyopathy may lead to left ventricular dysfunction, cardiogenic shock, dynamic left ventricular tract obstruction, pericardial effusion and death.43Stress-Induced Cardiomyopathy—Considerations for Diagnosis and Management during the COVID-19 Pandemic.COVID-19 and Cardiogenic ShockCOVID-19 has been linked to a variety of cardiovascular complications, ranging from mild myocardial injury to devastating cardiogenic shock that can lead to cardiovascular death. Several studies have been conducted to better understand the relationship between COVID-19 and cardiogenic shock. In a large registry of patients hospitalized for COVID-19 infection (n=15,208), 12% developed some form of shock (cardiogenic, distributive, or mixed), with 0.7% experiencing cardiogenic shock.44Varshney AS Omar WA Goodrich EL et al.Epidemiology of Cardiogenic Shock in Hospitalized Adults With COVID-19: A Report From the American Heart Association COVID-19 Cardiovascular Disease Registry. These individuals were more likely to be male, have diabetes, a history of myocardial infarction or HF, have higher troponin levels, and lower left ventricular ejection fraction compared to those without shock.44Varshney AS Omar WA Goodrich EL et al.Epidemiology of Cardiogenic Shock in Hospitalized Adults With COVID-19: A Report From the American Heart Association COVID-19 Cardiovascular Disease Registry. Approximately 20% of those with cardiogenic shock had a myocardial infarction (including demand-related events) during the hospitalization.44Varshney AS Omar WA Goodrich EL et al.Epidemiology of Cardiogenic Shock in Hospitalized Adults With COVID-19: A Report From the American Heart Association COVID-19 Cardiovascular Disease Registry.Myocardial infarction is a known risk factor for developing cardiogenic shock, particularly ST-segment elevation myocardial infarction (STEMI). In the NACMI registry, 18% of STEMI patients with concomitant COVID-19 infection developed cardiogenic shock during the early phase of the pandemic,45Garcia S Dehghani P Grines C et al.Initial Findings From the North American COVID-19 Myocardial Infarction Registry. which decreased to 13% later in the pandemic.46Garcia S Dehghani P Stanberry L et al.Trends in Clinical Presentation, Management, and Outcomes of STEMI in Patients With COVID-19. Multiple mechanisms may increase the risk of cardiogenic shock in STEMI patients including delayed presentation, prolonged ischemic time, proinflammatory and prothrombotic effects, and cytokine storms.47Gorder K Young W Kapur NK et al.Mechanical Circulatory Support in COVID-19. The prognosis for these patients was poor, with in-hospital mortality risk being significantly higher in those with cardiogenic shock compared to those without shock in the AHA COVID-19 CVD Registry (63% vs. 10.3%, p44Varshney AS Omar WA Goodrich EL et al.Epidemiology of Cardiogenic Shock in Hospitalized Adults With COVID-19: A Report From the American Heart Association COVID-19 Cardiovascular Disease Registry. Similarly, cardiogenic shock increased the risk of in-hospital mortality by more than 4-fold in STEMI patients with concomitant COVID-19 infection in the NACMI registry.48Dehghani P Schmidt CW Garcia S et al.North American COVID-19 Myocardial Infarction (NACMI) Risk Score for Prediction of In-Hospital Mortality.Managing AMI-associated cardiogenic shock regardless of COVID-19 status is challenging, with standardized protocols including early revascularization and initial stabilization with or without mechanical circulatory support.49Henry TD Tomey MI Tamis-Holland JE et al.Invasive Management of Acute Myocardial Infarction Complicated by Cardiogenic Shock: A Scientific Statement From the American Heart Association. However, the evidence for the use of mechanical circulatory support in COVID-19 patients, particularly extracorporeal membrane oxygenation (ECMO), is limited to observational studies. In the NACMI registry, intra-aortic balloon pumping (IABP) was the most common form of mechanical circulatory support (62%), followed by Impella (28%), and ECMO (7%).50Guddeti RR Sanina C Jauhar R et al.Mechanical Circulatory Support in Patients With COVID-19 Presenting With Myocardial Infarction. Despite using these strategies, the in-hospital mortality rate was still 60%. A large international registry of the Extracorporeal Life Support Organization (ELSO) also found that using ECMO for circulatory support was associated with in-hospital mortality risk of 89% in patients with COVID-19 infection.51Barbaro RP MacLaren G Boonstra PS et al.Extracorporeal membrane oxygenation support in COVID-19: an international cohort stud
Comments (0)