
Remember me




Women treated with cervical conization for cervical intraepithelial neoplasia grade 2 or worse (CIN2+) continue to be at risk for persistence or recurrence of CIN2+ and developing invasive carcinoma.1,2 Most recurrent lesions are seen within 2 years after treatment, but the risk remains in the following years.3,4 Adequate follow-up is therefore crucial. Several factors are thought to predict the risk of recurrence, and follow-up programs have traditionally involved cervical smears and/or colposcopy. It is well known that women with involved resection margins have a higher risk of residual/recurrent CIN2+ than women with free margins.5,6 Recognition of high-risk human papillomavirus (HPV) as a causal factor for CIN and invasive cervical cancer has led to the addition of HPV testing to cytology in many follow-up programs. However, only a few studies on HPV testing alone have been published,7–11 and until today, there is still no international consensus on post-treatment surveillance strategies.
In Denmark, the postconization follow-up is described in national clinical guidelines under The Danish Health Authority.12,13 At the 1st follow-up visit 6 months after conization, a cotest with cytology and HPV test as test of cure (TOC) is performed. Depending on the resection margins and the result of the TOC, the women are allocated into 1 of 3 categories. Women with free resection margins and 1) normal cytology and negative HPV test results are returned to the national screening program; 2) atypical squamous cells of undetermined significance (ASCUS)/low-grade squamous intraepithelial lesion (LSIL) and/or positive HPV test results are recommended a repeated TOC after 6 months; and 3) high-grade squamous intraepithelial lesion (HSIL)/atypical squamous cells–cannot exclude HSIL/atypical glandular cells/adenocarcinoma in situ (AIS) and/or positive HPV test results are referred to colposcopy with biopsy. Women with involved or unclarified resection margins and 1) negative HPV test result and cytology normal/ASCUS/LSIL are recommended a repeated TOC after 6 months; 2) positive HPV test results and normal cytology are recommended a repeated TOC after 6 months; and 3) ASCUS/LSIL, and positive HPV, or atypical squamous cells–cannot exclude HSIL/HSIL/atypical glandular cells/AIS with any HPV result are referred to colposcopy with biopsy.12
The aim of our study was to assess if cytology can be omitted in the follow-up after treatment for CIN2+ and if HPV test can be used alone as TOC after stratifying for resection margin status.
MATERIAL AND METHODS Ethical ApprovalThe project was approved by the institutional review board (IRB) and the national Data Protection Agency. The requirement for written informed consent was waived by the IRB because the study was register-based.
ParticipantsThis population-based and register-based study included women who had a cervical conization performed in Danish hospitals between January 1 and December 31, 2013. The women were identified in The Danish Pathology Data Bank, a national online health care registry in Denmark containing information on all histological and cytological specimens handled by pathology departments in Denmark since the 1990s. The Danish Pathology Data Bank uses Systematized Nomenclature of Medicine, which has separate codes for topography, morphology, etiology, function, disease, and procedure. The topography code T83701 for cone was used to identify the study population. All Danish citizens have a unique, personal 10-digit identifier by which histology, cytology, and HPV test results for each woman were obtained for a 3-year follow-up period. Data from January 1 to December 31, 2012, were also obtained to validate a potential preconization biopsy for the women who had surgery in early 2013.
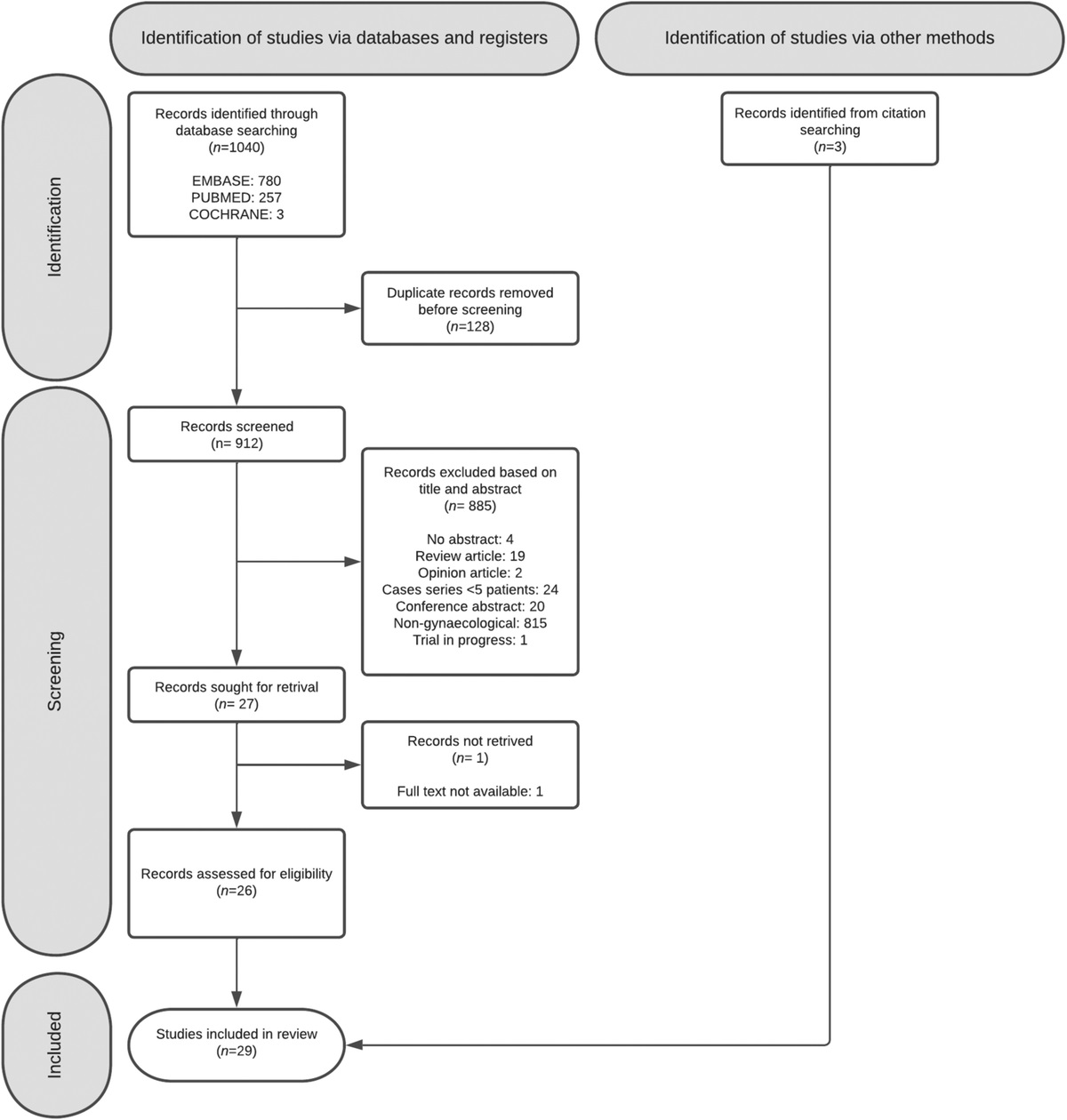
Women who had a cervical conization performed in Denmark between January 1 and December 31, 2013, were included. Women diagnosed with cancer in the cone or absent cytology and/or HPV test results postconization were excluded (Figure 1).
 FIGURE 1:
FIGURE 1: Study population.
Data included the women's age at time of surgery, histological diagnosis on potential preconization biopsy, and the cone resection, along with information about the resection margins of the cone. The postconization data were HPV test result, cytology, and/or biopsies.
The assay used for HPV testing was cobas 4800 System (Roche Diagnostics, Basel, Switzerland) in 4 of 5 regions in Denmark and digene HC2 High-Risk HPV DNA test (Qiagen, Hilden, Germany) in 1 region.14
Residual/recurrent disease was defined as histologically confirmed CIN2+ in the follow-up period. Cervical intraepithelial neoplasia grade 2 or worse includes CIN2, CIN3, AIS, adenocarcinoma (AC), and squamous cell carcinoma (SCC).
Resection margins were defined as involved when CIN2+ occurred. If the resection margins were unclear or not evaluated, they were defined as involved margins as per the recommendations of the Danish National Board of Health. Human papillomavirus types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68 were defined as HPV positive. The finding of ASCUS or worse (ASCUS+) was defined as cytology positive.
On January 1, 2013, the recommendations from the Danish National Board of Health for follow-up after treatment of precursor lesions was implemented, by which a combination of cytology and HPV-DNA testing stratified by resection margin status was performed. When the result was negative HPV test and normal cytology after free resection margins at follow-up 6 months after conization, the women were recommended to return to the national screening program. Should any of the 3 parameters be abnormal, the recommendation was to continue the follow-up program with control at a gynecologist every 6 to 12 months depending on the results.13
Statistical AnalysesCharacteristics of the population were summarized using descriptive statistics. Pearson χ2 tests were performed to test for statistically significant (level 0.05) differences between the women with and without residual/recurrent disease. To investigate the agreement between single testing and cotesting predicting recurrent disease after conization, we estimated the sensitivity (SN), specificity (SP), positive predictive value (PPV), and negative predictive value (NPV) with exact binomial 95% CI for HPV, margins, and cytology, a combination where at least 1 test was positive. All statistical analyses were performed in Stata, version 15.0 (StataCorp, College Station, TX).
RESULTSThe study identified 5,174 women who had a cervical conization performed at a Danish hospital in 2013 and followed up with HPV test and cytology at first control visit (Figure 1). Characteristics of the study population are listed in Table 1. The median age of the 5,174 women was 33.8 years (interquartile range [IQR] = 27.5–41.5).
TABLE 1 - Characteristics of the Study Population Total (n = 5,174) No Residual/Recurrent Disease (n = 4,856) Residual/Recurrent Disease (n = 318) p Age (median ± IQR) 33.8 (27.5–41.5) 33.5 (27.5–41.3) 37.4 (30.3–45.7) <.001 Pathology at conization <.001 Normal 365 (7.1) 341 (7.0) 24 (7.6) CIN NOS 139 (2.7) 136 (2.8) 3 (0.9) CIN1 337 (6.5) 331 (6.8) 6 (1.9) CIN2 957 (18.5) 921 (19.0) 36 (11.3) CIN3 3,168 (61.2) 2,938 (60.5) 230 (72.3) AIS 197 (3.8) 180 (3.7) 17 (5.4) Other/NA 11 (0.2) 9 (0.2) 2 (0.6) Margins <.001 Free 2,780 (53.7) 2,707 (55.8) 73 (23.0) Involved 2,394 (46.3) 2,149 (44.2) 245 (77.0) High risk HPV (follow-up) <.001 Negative 3,711 (71.7) 3,659 (75.3) 52 (16.3) Positive 1,463 (28.3) 1,197 (24.7) 266 (83.7) Cytology (follow-up) <.001 Normal 4,426 (85.5) 4,320 (89.0) 106 (33.3) ASCUS+ 748 (14.5) 536 (11.0) 212 (66.7)IQR indicates interquartile range; NA, not available; NOS, not otherwise specified.
In 83.5% (4,322/5,174) of the total study population, CIN2+ was detected in the cone, whereas 16.5% (852/5,174) had normal histology, unclassified CIN, and CIN1. A total of 53.7% (2,780/5,174) of the women had free resections margins. Margins were categorized as involved in 46.3% (2,394/5,174) as per recommendation of the Danish National Board of Health (Table 2). Of these, 1,415 were histologically verified as involved, and in 979, the margins were unclear or not evaluated. Residual/recurrent disease was most frequently seen in the cases with histologically involved margins (13.6%) compared with unclear/not evaluated (5.2%) margins.
TABLE 2 - Characteristics of the 5,174 Women According to Resection Margins Free Resection Margins (n = 2,780) Involved Resection Margins (n = 2,394) Age (median ± IQR) 33.8 (27.5–41.7) 33.7 (27.6–41.2) Biopsy Normal 122 (4.4) 48 (2.0) CIN NOS 133 (4.8) 101 (4.2) CIN1 123 (4.4) 80 (3.3) CIN2 643 (23.1) 504 (21.0) CIN3 1,584 (57.0) 1,479 (61.8) AIS 81 (2.9) 96 (4.0) AC 1 (0.1) 1 (0.1) SSC 3 (0.1) 2 (0.1) Other/NA 90 (3.2) 83 (3.5) Pathology at conization Normal 365 (13.1) — CIN NOS 60 (2.2) 79 (3.3) CIN1 201 (7.2) 136 (5.6) CIN2 552 (19.9) 405 (16.9) CIN3 1,524 (54.8) 1,644 (68.7) AIS 78 (2.8) 119 (5.0) Other/NA — 11 (0.5) Combined testing HPV+/Cyt+ 168 (6.0) 347 (14.5) HPV+/Cyt− 502 (18.1) 446 (18.6) HPV−/Cyt+ 102 (3.7) 131 (5.5) HPV−/Cyt− 2,008 (72.2) 1,470 (61.4) Disease in follow-up 73 (2.6) 245 (10.2) CIN2 37 63 CIN3 33 159 AIS 3 15 AC — 1 SSC — 7Most of the population (93.9%, 4,856/5,174) had no residual/recurrent disease during the 3-year follow-up period in the study, but histologically confirmed CIN2+ (residual/recurrent disease) was observed in 6.1% (318/5,174) of the women. The women with recurrent disease were slightly older (median 37.4 years [IQR = 30.3–45.7]) than the women without recurrent disease (median 33.5 years [IQR = 27.5–41.3]). Of the women with residual/recurrent disease, the margins were involved in 77.0% (245/318) compared with 44.2% (2,149/4,856) in the group without residual/recurrent disease. A positive HPV test was found in 83.7% (266/318) and 24.7% (1,197/4,856) of the 2 groups respectively, and 66.7% (212/318) versus 11.0% (536/4,856) had ASCUS+.
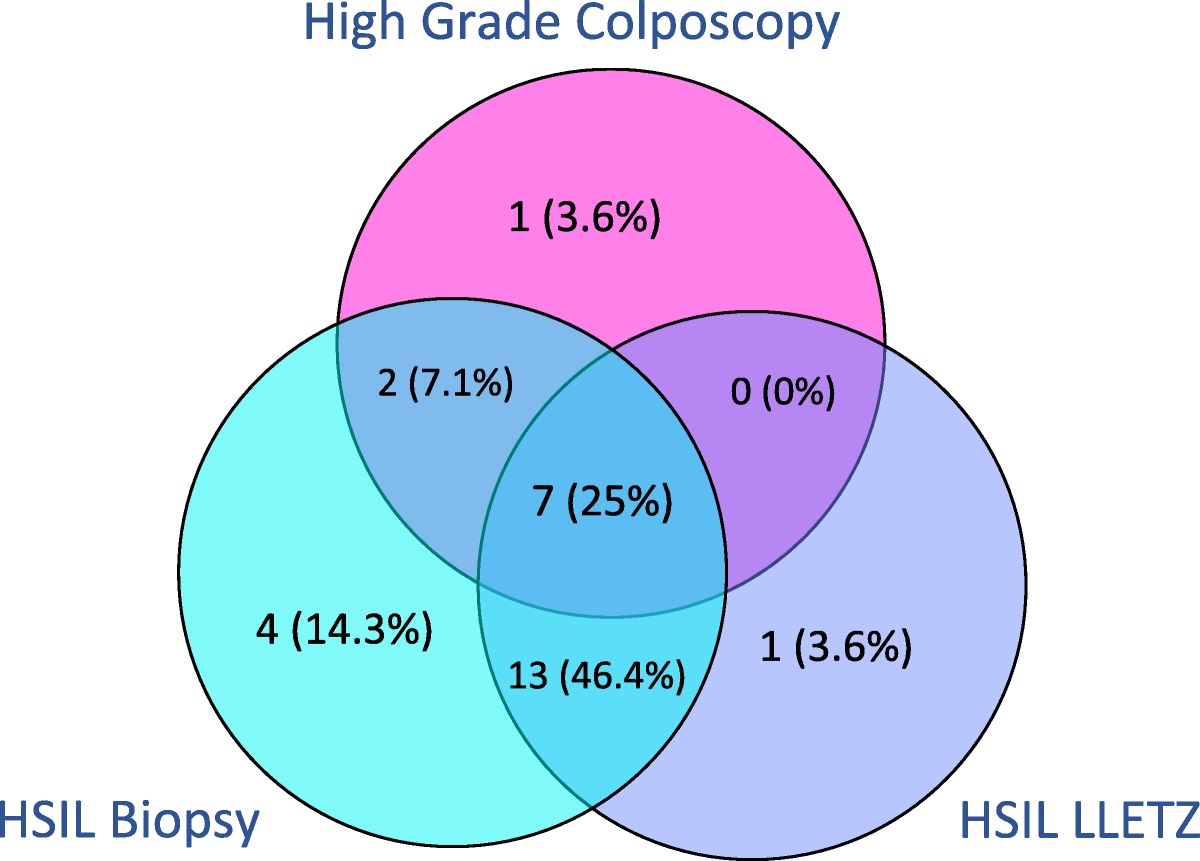
The distribution of residual/recurrent disease related to margin status and follow-up results are shown in Figure 2. In the group with margins+/HPV+/cytology+, 43.8% (152/347) had residual/recurrent disease (39 CIN2, 101 CIN3, 6 AIS, 1 AC, and 5 SCC). By comparison, in the group with margins−/HPV−/cytology−, only 0.4% (9/2,008) had residual/recurrent disease (5 CIN2 and 4 CIN3). The follow-up results of the group with margins− shows that 13 of 2,780 (0.5%) with HPV− had residual/recurrent disease and 9 of 2,780 (0.3%) when cytology− was added, and there were no cancers in this group. On the other hand, in the margin+/HPV− group, 1.6% (39/2,394) had residual/recurrent disease and 0.9% (22/2,394) when cytology− was added, and there were 2 SCC.
 FIGURE 2:
FIGURE 2: Distribution of recurrent disease in the study population. Margins+ defined as involved margins (CIN2+, also including unclear or not evaluated). HPV+ defined as high-risk HPV types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and/or 68. Cytology+ defined as atypical squamous cells of unknown significance or worse.
In total, 8 women developed carcinoma during the 3-year follow-up. Most (6/8) were identified in the margin+/HPV+/cytology+ group and 2 women in the margin+/HPV−/cytology− group. The median age for the 8 women with carcinoma was 49.6 years (IQR = 34.3–57.3) compared with the study population's median age of 33.8 (IQR = 27.5–41.3).
Table 3 shows the rate and distribution of residual/recurrent disease according to time for first follow-up, where HPV test and cytology were done for the entire study population. The guidelines recommend first control at 6 months. A total of 70.9% (3,667/5,174) had first control within 6 months after conization (defined as <7 mo), and 19.6% (1,014/5,174) had first control at ≥7 and <12 months. The remaining 9.5% (493/5,174) had first control ≥12 months after conization with a median of 16.5 months (IQR = 13.7–21.7).
TABLE 3 - Residual/Recurrent Disease According to Time for First Follow-Up Visit, Where HPV Test and Cytology Were Done Residual/Recurrent disease Time for First Follow-Up Visit (n = 5,174) <7 mo ≥7 & < 12 mo ≥12 mo No 3,429 954 473 Yes 238 60 20 CIN2 79 13 8 CIN3 145 41 8 AIS 10 5 3 AC 0 0 1 SCC 6 1 0The SN, SP, PPV, and NPV for different TOC strategies to predicting recurrent disease after conization are listed in Table 4. Using HPV test as standalone TOC after stratifying for margins status, the SN, SP, PPV, and NPV were 95.9%, 43.2%, 10.0%, and 99.4%, respectively, and for combined testing (margin status, HPV, and cytology) 97.2%, 41.2%, 9.8%, and 99.6%, respectively.
TABLE 4 - Sensitivity, Specificity, PPV, and NPV for Different Testing Strategies for CIN2+ in Follow-Up for 5,174 Women No. Tested Positive Sensitivity % (95% CI) Specificity % (95% CI) Positive Predictive Value % (95% CI) Negative Predictive Value % (95% CI) Margins/HPV/cytology 3,401 97.2 (94.7–98.7) 41.2 (39.8–42.6) 9.8 (8.8–10.9) 99.6 (99.2–99.8) Margins/HPV 3,313 95.9 (93.1–97.8) 43.2 (41.8–44.6) 10.0 (8.9–11.1) 99.4 (98.9–99.7) HPV 1,463 83.7 (79.2–87.6) 75.4 (74.1–76.6) 18.3 (16.3–20.3) 98.6 (98.2–99.0) Cytology 748 66.8 (61.3–71.9) 89.0 (88.1–89.8) 28.5 (25.3–31.9) 97.6 (97.1–98.0)Threshold for positivity:
Margins+: margins involved, unclear or not evaluated (as per the recommendations of the Danish National Board of Health). HPV+: HPV types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68. Cytology +: ASCUS or worse (ASCUS+). Residual/recurrent disease: histologically confirmed CIN2+ (CIN2, CIN3, AIS, AC, and SCC).
In this register-based study, we find that TOC with HPV test at the first post-treatment follow-up visit after stratifying for resection margins has an equally high sensitivity and NPV as combined testing with cytology and HPV. In the group with free resection margins, very few patients had residual/recurrent disease if HPV was negative or both HPV and cytology were negative (0.5% vs 0.3%).
A total of 6.1% had residual/recurrent disease in the 3-year follow-up period. This is in line with other studies showing recurrency rates between 3.6% and 6.6%.6,10,15–18
In a population-based study with 10-year follow-up, 2.5% of HPV− women had recurrent disease,9 and a prospective 5-year study found no women with recurrence in the HPV− group and 12.3% in the HPV+ group.11 Our finding of 1.4% (52/3,711) of HPV− women with residual/recurrent disease and 18.2% (266/1,463) of HPV+ women with residual/recurrent disease are equivalent to this.
Combined testing has been implemented in many follow-up programs during the last decade, and the question whether HPV test can be used as a standalone TOC is still being discussed. Some studies provide data showing that the diagnostic accuracy of HPV test alone is similar to cotesting with cytology and HPV.19–21 A recent systematic review and metaanalysis demonstrated that cotesting with HPV/cytology only provides a small reduction in risk of CIN2+ compared with HPV test alone at the cost of a higher test positivity.22 A Japanese study, with pooled data from 33 published articles including a total of 5,319 women, finds equal sensitivity and NPV for HPV test alone and cotesting (92% vs 93% and 99% vs 99%, respectively).21 Other studies argue that HPV could be used as a standalone TOC after conization. A Danish study of 477 women found that adding cytology to a negative HPV test at the first post-treatment control did not improve the detection of residual/recurrent CIN2+ in long-term follow-up.9 A large Canadian study of 2,340 women concluded that women with a negative HPV test 12 months post-treatment can safely return to annual routine screening.10 In an Italian study, the authors concluded that HPV DNA testing at 6 months after treatment for CIN2+ effectively identifies women who are disease-free with an NPV of 100% at 5-year follow-up and suggested that the women can return to annual cytological testing after just a single follow-up 18 months post-treatment.11
There is no consensus on whether resection margins status should be included in follow-up. The Japanese study21 found that women with margin+/HPV+ had a 67.5% risk of post-treatment CIN2+ versus only 1.3% risk in women with margin+/HPV− and 0.9% risk in women with margin−/HPV− and concluded that HPV testing may be used for identifying populations with different risks, especially in women with involved margins. The most recent metaanalysis including more than 40,000 women found that even though the risk of residual or recurrent CIN2+ is higher when resection margins are involved, a post-treatment HPV test predicts treatment failure more accurately than margin status.6 However, a recent large prospective Swedish study including almost a thousand women found that women with margins+/HPV+ have a greater than 2.5-fold risk of recurrent disease compared with women with margins−/HPV+ and concluded that margin status combined with HPV test increase the accuracy for predicting treatment failure.5 The importance of and benefits from looking at both the margin status and HPV in follow-up are becoming evident.16 Our findings support that HPV test as TOC after stratifying for margins status is effective and sufficient to identify the woman at risk for residual/recurrent disease.
In our study, 0.15% (8/5,174) developed carcinoma during follow-up; 6 women had FIGO stage IA1 and 2 had FIGO stage IB1 disease, indicating that the follow-up program fulfilled its purpose and only few severe recurrences were seen. In each of the 8 cases, the margins were involved, and 6 were in the margin+/HPV+/cytology+ group, whereas 2 were in the margin+/HPV−/cytology− group. The 2 women who had negative HPV test results were slightly older than the median study population (aged 50 and 54 years). Sampling error because of the gradual retraction of the transformation zone from exocervix to endocervix with age23 could be a possible explanation for the negative HPV test result and negative cytology. A concern for false negatives, as also raised in a smaller retrospective study,19 is reasonable because this could result in a woman with residual/recurrent disease terminating the follow-up too early. However, the risk should be seen in the light of what subsequences the follow-up. In most countries, the women return to a routine screening program after follow-up. The screening programs differ in screening intervals, screening methods used, and age groups included. This should be taken in consideration when evaluating at what point it is safe to return to routine screening after completing a follow-up program after treatment for CIN2 +.
The main goal of a follow-up program should be to identify not only women who have residual/recurrent disease but also women who are not at risk. One could argue that a high sensitivity and NPV is more important than specificity and PPV if adherence to routine screening after follow-up is expected. The current study shows that the diagnostic performance of HPV testing alone was good with high sensitivity and NPV. Especially in the group with free resection margins, where only 0.5% had residual/recurrent disease, HPV test as TOC is useful. Moreover, in the group with involved margins, the risk of recurring CIN2+ was low (1.6%) when using HPV test as TOC. However, because 2 women developed carcinoma in this group and CIN2+ is found in the group with HPV−/cytology+, we recommend to still follow the current Danish recommendation with repeated TOC with cotest (HPV and cytology) at 6 and 12 months for women with involved margins. This implicates using different testing strategies depending on margin status: HPV test alone as TOC when margins are free and still using cotest (HPV and cytology) when margins are involved.
The large sample size is a major strength in our study. Furthermore, the study is a national population-based and register-based study using valid and robust data from The Danish Pathology Data Bank.24 Even though the recommendations on follow-up were implemented just 1 year before the study, the adherence was high because more than 90% of the women who had a conization performed in 2013 had both cytology and HPV test at first post-treatment control and 70.9% of the women attending the first postconization control <7 months.
A 3-year follow-up could be considered a limitation to the study. We, however, chose this because it is known that the risk for recurrent/residual disease lowers through the years, and we wished to test the effect of the follow-up program. Had the period been longer, there would have been a risk for de novo disease.
The proportion of women with margins defined as involved might seem high compared with previous studies.6 This is because of the fact that unclear or not evaluated margins is defined as involved as per the recommendations of the Danish National Board of Health, with the purpose of offering these women a second follow-up visit at 12 months for safety reasons.
Data on excision type used, size of excision, and test platform used for HPV testing were not reported systematically in The Danish Pathology Data Bank and could therefore not be analyzed in this study.
Overall, the study is, however, a representative picture of the current setting in Denmark, and the results can be extrapolated to similar populations and comparable screening programs.
CONCLUSIONSIn conclusion, we suggest it might be safe to use HPV test alone as TOC for CIN2+ after stratifying for resection margin status. This strategy yields a comparably high SN and NPV as cotesting with cytology and HPV test. In the group with free resection margins, 1 TOC with HPV test alone at 6 months is sufficient, but in the group with involved margins, TOC as cotest with HPV and cytology are recommend.
ACKNOWLEDGMENTSThe authors thank Jalil Hariri, MD, for providing inspiration to the study.
REFERENCES 1. Kocken M, Helmerhorst TJ, Berkhof J, et al. Risk of recurrent high-grade cervical intraepithelial neoplasia after successful treatment: a long-term multi-cohort study. Lancet Oncol 2011;12:441–50. 2. Strander B, Hallgren J, Sparen P. Effect of ageing on cervical or vaginal cancer in Swedish women previously treated for cervical intraepithelial neoplasia grade 3: population based cohort study of long term incidence and mortality. BMJ 2014;348:f7361. 3. van Hamont D, van Ham MA, Struik-van der Zanden PH, et al. Long-term follow-up after large-loop excision of the transformation zone: evaluation of 22 years treatment of high-grade cervical intraepithelial neoplasia. Int J Gynecol Cancer 2006;16:615–9. 4. Arbyn M, Ronco G, Anttila A, et al. Evidence regarding human papillomavirus testing in secondary prevention of cervical cancer. Vaccine 2012;30:F88–99. 5. Alder S, Megyessi D, Sundström K, et al. Incomplete excision of cervical intraepithelial neoplasia as a predictor of the risk of recurrent disease-a 16-year follow-up study. Am J Obstet Gynecol 2020;222:172.e1–172.e12. 6. Arbyn M, Redman CWE, Verdoodt F, et al. Incomplete excision of cervical precancer as a predictor of treatment failure: a systematic review and meta-analysis. Lancet Oncol 2017;18:1665–79. 7. Strander B, Ryd W, Wallin KL, et al. Does HPV-status 6–12 months after treatment of high grade dysplasia in the uterine cervix predict long term recurrence?Eur J Cancer 2007;43:1849–55. 8. Katki HA, Schiffman M, Castle PE, et al. Five-year risk of recurrence after treatment of CIN 2, CIN 3, or AIS: performance of HPV and Pap cotesting in posttreatment management. J Low Genit Tract Dis 2013;17:S78–84. 9. Gosvig CF, Huusom LD, Andersen KK, et al. Long-term follow-up of the risk for cervical intraepithelial neoplasia grade 2 or worse in HPV-negative women after conization. Int J Cancer 2015;137:2927–33. 10. Ceballos KM, Lee M, Cook DA, et al. Post-loop electrosurgical excision procedure high-risk human papillomavirus testing as a test of cure: the British Columbia experience. J Low Genit Tract Dis 2017;21:284–8. 11. Garutti P, Borghi C, Bedoni C, et al. HPV-based strategy in follow-up of patients treated for high-grade cervical intra-epithelial neoplasia: 5-year results in a public health surveillance setting. Eur J Obstet Gynecol Reprod Biol 2017;210:236–41. 12. Petersen LK. National klinisk retningslinje for celleforandringer på livmoderhalsen. 2019. Available at: https://www.sst.dk/da/Viden/Sundhedsvaesen/NKR-og-NKA/Puljefinansierede-NKR/Celleforandringer-paa-livmoderhalsen. Accessed February 15, 2022. 13. Sundhedsstyrelsen. Screening for livmoderhalskræft. Anbefalinger 2012. Summary in English. 2012. Available at: http://www.sst.dk/~/media/B1211EAFEDFB47C5822E883205F99B79.ashx. Accessed February 15, 2022. 14. DKLS. Dansk Kvalitetsdatabase For Livmoderhalskræftscreening - Årsrapport 2013. 2014. Available at: https://danskcytologiforening.dk/dkls/2013/DKLS%202013.pdf. Accessed February 15, 2022. 15. Ryu A, Nam K, Kwak J, et al. Early human papillomavirus testing predicts residual/recurrent disease after LEEP. J Gynecol Oncol 2012;23:217–25. 16. Bruhn LV, Andersen SJ, Hariri J. HPV-testing versus HPV-cytology co-testing to predict the outcome after conization. Acta Obstet Gynecol Scand 2018;97:758–65. 17. Gosvig CF, Huusom LD, Deltour I, et al. Role of human papillomavirus testing and cytology in follow-up after conization. Acta Obstet Gynecol Scand 2015;94:405–11. 18. Fernández-Montolí ME, Tous S, Medina G, et al. Long-term predictors of residual or recurrent cervical intraepithelial neoplasia 2–3 after treatment with a large loop excision of the transformation zone: a retrospective study. BJOG 2020;127:377–87. 19. Mo LZ, Song HL, Wang JL, et al. Pap smear combined with HPV testing: a reasonable tool for women with high-grade cervical intraepithelial neoplasia treated by LEEP. Asian Pac J Cancer Prev 2015;16:4297–302. 20. Kocken M, Uijterwaal MH, de Vries AL, et al. High-risk human papillomavirus testing versus cytology in predicting post-treatment disease in women treated for high-grade cervical disease: a systematic review and meta-analysis. Gynecol Oncol 2012;125:500–7. 21. Onuki M, Matsumoto K, Sakurai M, et al. Posttreatment human papillomavirus testing for residual or recurrent high-grade cervical intraepithelial neoplasia: a pooled analysis. J Gynecol Oncol 2016;27:e3. 22. Clarke MA, Unger ER, Zuna R, et al. A systematic review of tests for postcolposcopy and posttreatment surveillance. J Low Genit Tract Dis 2020;24:148–56. 23. Autier P, Coibion M, Huet F, et al. Transformation zone location and intraepithelial neoplasia of the cervix uteri. Br J Cancer 1996;74:488–90. 24. Erichsen R, Lash TL, Hamilton-Dutoit SJ, et al. Existing data sources for clinical epidemiology: the Danish National Pathology Registry and Data Bank. Clin Epidemiol 2010;2:51–6.
Comments (0)