
Remember me





Oxygen is one of the most common and inexpensive treatment components in today's world of modern medicine. It is the most essential medicinal gas available in the majority of the hospitals and highly beneficial when used in appropriate amounts. However, it must be acknowledged that too much of anything tends to do more harm than good, and even oxygen therapy is no exception.
When one talks about oxygen, hypoxia and hypoxemia are two such terminologies often interchangeably encountered and used. It is of paramount importance to note these two terminologies, though they may overlap and are not synonymous. Hypoxia is a state of insufficient amount of oxygen in the tissues, whereas hypoxemia is a decreased amount of oxygen content in the blood. Hypoxemia may often go unnoticed, and when homeostatic mechanisms no longer compensate, it can lead to hypoxia.1
With the ongoing COVID-19 pandemic, oxygen utilization has been on the rise worldwide, with some countries often experiencing scarcity in such crucial times.2 The goal of oxygen therapy in COVID-19, as with any other form of respiratory illness, is to treat hypoxia. The WHO has classified severe COVID-19 to have saturations less than 90% and thus warranting supplemental oxygen therapy.3 In an effort to treat the hypoxia, prolonged oxygen therapy may lead to pathophysiological processes associated with increased levels of hyperoxia-induced reactive oxygen species (ROS), which may readily react with surrounding biological tissues causing protein denaturation and breaking down of nucleic acids into strands.4 In this study, we describe a case of a patient with COVID-19 treated at our hospital.
2 CASE PRESENTATIONA 64-year-old man with hypothyroidism, on a daily dose of levothyroxine 100 mcg, presented to our emergency department with the complaint of difficulty in breathing of gradual onset and progressive in nature for the past 5 days associated with chest tightness. He denied the presence of any other symptoms. He had a history of coming into contact with COVID-19 patients and a history of domestic travel within the country in the last two weeks.
The only abnormal findings on physical examination were oxygen saturations of 79% on room air and tachypnea of 26 breaths/min. Blood pressure and heart rate on arrival were 124/71 mm Hg and 101 beats per minute, respectively. Chest auscultation revealed anterior bilateral basal crackles, and the entirety of the posterior, superior, and inferior aspects had crackles. It was noted that the patient experienced fatiguability on moderate exertion, however, had no difficulty in completing sentences.
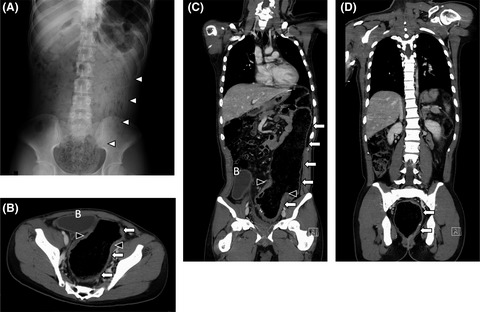
Chest X-ray (PA and lateral views) was performed and revealed bilateral peripheral and central alveolar infiltrates suggestive of atypical pneumonia (Figure 1). Nasal swab PCR test for COVID-19 was positive. A series of blood investigations were performed on days 1, 3, 5, and 7 of hospital stay (Table 1).

Bilateral peripheral and central alveolar infiltrates on chest X-ray
TABLE 1. Table of results Investigation Day 1 Day 3 Day 5 Day 7 WBC (10 × 9/L) 13.4 16.4 16.1 9.3 NEU (10 × 9/L) 11.8 14.2 12.1 6.2 LYM (10 × 9/L) 1.1 0.4 2.2 2.4 PLT (10 × 9/L) 240 315 403 294 HB (g/dl) 15.7 15.4 15.8 15.2 BUN (mmol/L) 4.5 7.9 4.9 5.1 Creatinine (μmol/L) 117 182 98 102 Ferritine (ng/ml) 521 3000 2022 298 D-DIMER (mg/L) 2.7 – 0.04 0.03 Albumin (g/L) 36 42 30 34 Na (mmol/L) 141 141 137 141 K (mmol/L) 3.7 4.6 3.4 3.6 Cl (mmol/L) 103 106 98 105It was exceptional and noteworthy that throughout his hospital stay, the patient was never supplemented with any oxygen but continued with pharmacological therapies. The patient was on intravenous ceftriaxone 2 g once a day, methylprednisolone 125 mg, oral azithromycin 500 mg, and colchicine 1 mg once a day. He was also on oral multivitamin and mineral supplements throughout his hospital stay and continued after discharge. He was initiated on a heparin infusion of 2,000 IU/h for 5 days, along with warfarin 5 mg once a day. He also received a stat dose of tocilizumab 600 mg on day 3 of his admission. Chest physiotherapy using a spirometer was encouraged and along with awake prone positioning 6–12 h.
From day 5 onward, the trend of results showed an improvement in numbers and likewise clinical improvement was noted in the patient along with the subsiding of chest tightness and fatiguability. Tachypnea subsided over time returning the patient to an almost normal respiratory rate, and room air oxygen saturations showed some improvement, with the highest levels recorded being 92%, constant up to the point of discharge and for isolation at home on day 8 since admission.
3 DISCUSSIONPatients who presented to our hospital with COVID-19-related respiratory distress have had varying forms of oxygen supplementation ranging from those with mild distress on nasal cannulas to those with severe acute respiratory distress syndrome (ARDS) on invasive mechanical ventilation. The only variation in the treatment of this patient as opposed to others was oxygen. The patient in this case was never once supplemented with any oxygen for the entire duration of admission. The reason for withholding supplemental oxygen was the relative clinical stability of this patient despite presenting with hypoxemia. Prior to this case, we had observed several patients with similar clinical presentation who were supplemented with oxygen to meet a required high-set oxygen target. Eventually, they ended up having a prolonged hospital stay with an increased oxygen demand over time. Long-term exposure to high levels of oxygen can cause lung injury in the absence of mechanical ventilation, but the combination of these two becomes more lethal leading to further lung damage.5
During viral respiratory illnesses, ROS are necessary for eradicating viruses, thus aiding immune cells in phagocytosis function and in signal transduction. Excessive oxygenation can cause the amount of ROS to exceed the required redox homeostasis leading to histologically progressive destruction of alveolocapillary membranes causing obstruction of capillaries forming microthrombi and air leaks via already injured alveoli into the surrounding tissues.6 Eventually, prolonged iatrogenic exposure to oxygen in combination with COVID-19 can exacerbate cell apoptosis at the alveolar epithelium level resulting in pulmonary fibrosis over an extended time period.7
Lung tissues are protected by overactive immune-mediated adenosine A2A receptor cells. These immune cells play a critical role in the downregulation of pulmonary inflammation. Uncontrolled pulmonary inflammation occurs when a continuous amount of oxygen is administered that weakens the adenosine A2A receptor-mediated anti-inflammatory mechanism, thereby further exacerbating lung damage.8 A study performed on a small population receiving inhaled adenosine showed promising results in patients with COVID-19 in an attempt to therapeutically compensate for the oxygen-related loss of the endogenous adenosine receptor (A2AR)-mediated cells and reduce the lung destructing inflammatory process.9
Most pulmonary- and nonpulmonary-related studies recommend that no oxygen supplementation is required when oxygen saturation is more than 92%. Oxygen supplementation should start only if oxygen saturation is less than 90%.10 However, no consensus has yet been established on what the oxygenation target should be in hypoxemic respiratory failure patients.11
A meta-analysis study published even before the COVID-19 pandemic described that hyperoxia for a duration of more than 12–24 h often led to serious deleterious side effects. It was also noted that hyperoxia of even shorter durations may be associated with increased morbidity and mortality in ICU patients.12 The mortality rates of acutely ill adults in multiple clinical syndromes were lower in those who received conservative amount of oxygen as opposed to the liberal batch.13
Recent observation proposes no direct evidence of the benefit of providing supplemental oxygen therapy in the absence of hypoxia in COVID-19 patients such as in patients with low oxygen saturations who are perfectly comfortable or rather, “happy hypoxemic.” It may be used to wean patients off ventilatory support, but its use on patients whose lungs have adapted to hypoxemia or who do not require invasive therapy may in turn lead to adverse consequences.2 Overcorrecting hypoxemia may improve it in the short term, but its long-term effects can lead to oxygen-induced ARDS and ventilator-associated lung injury. These data suggest that the lungs have a better chance of recovery from COVID-19 when exposed to less oxygenation and invasive ventilation. Permissive hypoxemia was found to be feasible and had a better patient outcome when focused on oxygen content (CaO2) rather than oxygen saturations (SaO2).14
Based on these oxygen studies and our observation of patients, we could postulate that in patients undergoing a cytokine storm due to COVID-19, prolonged and excessive oxygen therapy adds insult in the form of oxygen reactive species to an already injured lung. We do not know whether this is an isolated case among millions or whether depriving this patient of oxygen did indeed work to his benefit. COVID-19 pneumonia of no doubt requires some form of oxygen, but the conundrum lies with those presenting with a mild form of respiratory distress, who despite having low saturations have minimal to no discomfort. COVID-19 respiratory distress presents with an unconventional pathogenesis in terms of hypoxemic patients and their progression to ARDS. Oxygen can do both heal and harm, and in the setting of COVID-19, which is still a new evolving disease, the question is not really about whether or not oxygen is required but rather how much is required.
4 CONCLUSIONSCondemning the use of oxygen in patients undergoing respiratory distress, be it from COVID-19 or any other illness is not the aim of this report. We are inquisitive to understand the role of oxygen in the treatment of COVID-19 and how best to titrate and use it to our benefit. Various studies have indeed been performed on the beneficial and detrimental effects of oxygen but not in the context of severe ARDS or pneumonia in relation to COVID-19. It is our hope that this case will inspire the need for further research using a bigger sample size to determine how much oxygen is too much in this new disease.
ACKNOWLEDGMENTSWe thank the Emergency, HDU, and ICU team of the Shree Hindu Mandal Hospital (SHMH) for their involvement in the treatment and care of this patient. We are grateful to our SHMH administrative team for giving us their support during the hardest times of the pandemic and having faith in us.
CONFLICT OF INTERESTNone declared.
AUTHOR CONTRIBUTIONSKishan Chudasama gathered the data and wrote the original draft. Esmail Sangey and Kishan Chudasama involved in editing of the manuscript. Esmail Sangey involved in supervision and submission of the manuscript. All took care of the patient and have approved the final version of the manuscript.
CONSENTInformed and written consent was obtained from the patient to publish in this case report.
The data that support the findings of this study are openly available in Authorea at https://doi.org/10.22541/au.163560986.68564911/v1
REFERENCES
1Bhutta BS, Alghoula F. Hypoxia. In: S Dulebohn, S Hauber, eds. StatPearls [Internet]. reasure Island, FL: StatPearls Publishing; 2021: 1– 17. Available from: http://www.ncbi.nlm.nih.gov/books/NBK482316/ 2Goyal DK, Mansab F, Bhatti S. Room to Breathe: The Impact of Oxygen Rationing on Health Outcomes in SARS-CoV2. Front Med. 2021; 7: 573037. doi:10.3389/fmed.2020.573037 3 COVID-19 Clinical management: living guidance [Internet]. [cited 2021 Oct 6]. Available from: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-clinical-2021-1 4Mach WJ, Thimmesch AR, Pierce JT, Pierce JD. Consequences of hyperoxia and the toxicity of oxygen in the lung. Nurs Res Pract. 2011; 5(2011):e260482. 5Roan E, Wilhelm K, Bada A, et al. Hyperoxia alters the mechanical properties of alveolar epithelial cells. Am J Physiol - Lung Cell Mol Physiol. 2012; 302(12): L1235- L1241. 6Chernyak BV, Popova EN, Prikhodko AS, Grebenchikov OA, Zinovkina LA, Zinovkin RA. COVID-19 and oxidative stress. Biochem Biokhimiia. 2020; 85(12): 1543- 1553. 7Fukumoto J, Leung J, Cox R, et al. Oxidative stress induces club cell proliferation and pulmonary fibrosis in Atp8b1 mutant mice. Aging. 2019; 11(1): 209- 229. 8Thiel M, Chouker A, Ohta A, et al. Oxygenation inhibits the physiological tissue-protecting mechanism and thereby exacerbates acute inflammatory lung injury. PLoS Biol. 2005; 3(6): e174. 9Correale P, Caracciolo M, Bilotta F, et al. Therapeutic effects of adenosine in high flow 21% oxygen aereosol in patients with Covid19-pneumonia. PLoS One. 2020; 15(10):e0239692. 10Moss BJ, Sargsyan Z. Things we do for no reason: supplemental oxygen for patients without hypoxemia. J Hosp Med. 2020; 14(4): 242- 244. 11Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021; 47(11): 1181- 1247. doi:10.1007/s00134-021-06506-y 12Hafner S, Beloncle F, Koch A, Radermacher P, Asfar P. Hyperoxia in intensive care, emergency, and peri-operative medicine: Dr. Jekyll or Mr. Hyde? A 2015 update. Ann Intensive Care. 2015; 5(1): 42. 13Chu DK, Kim LH-Y, Young PJ, et al. Mortality and morbidity in acutely ill adults treated with liberal versus conservative oxygen therapy (IOTA): a systematic review and meta-analysis. Lancet Lond Engl. 2018; 391(10131): 1693- 1705. 14Voshaar T, Stais P, Köhler D, Dellweg D. Conservative management of COVID-19 associated hypoxaemia. ERJ Open Res. 2021; 7(1): 00026- 2021.
Comments (0)