
Remember me


Thymic carcinoma is an epithelial tumor derived from thymic epithelial cells, the most common types of which are squamous cell carcinoma, spindle cell, lymphoepithelial-like and basaloid carcinoma.1 Among thymic tumors, thymic carcinoma has been reported to have a significantly lower survival rate due to its aggressive behavior. Higher overall survival (OS) and recurrence-free survival (RFS) rates are related to tumor stage and a complete surgical resection.2 Thymic tumors may be associated with other simultaneous and/or metachronous extra-thymic tumors.3, 4 Based on the evidence in the literature, we report the case of a patient with a peculiar cancer history. He was previously diagnosed and surgically treated for prostatic adenocarcinoma and colic adenocarcinoma. During follow-up, in January 2019, lung cancer was diagnosed with simultaneous mediastinal suspected neoplasm. Uniportal video-assisted thoracic surgery (uni-VATS) is an established mini-invasive technique for both mediastinal and lung surgery. Compared with an open thoracotomy approach, its superiority is due to less postoperative complications and pain, shorter hospital stay and permanence of chest drain. On the other hand, the oncological results are equal to conventional thoracotomy.5-7 Considering the patient's age and comorbidities we performed concurrent surgery with a uni-VATS approach.
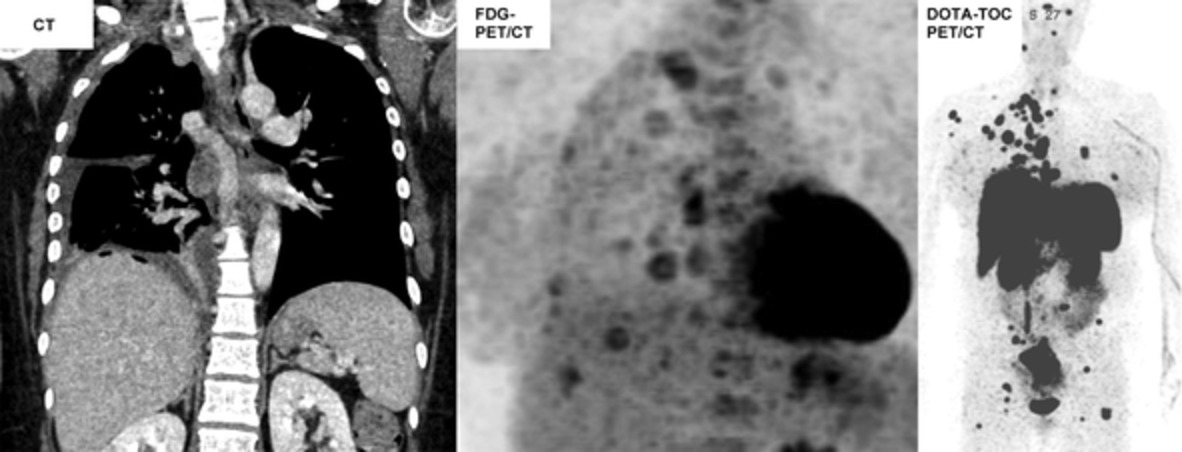
CASE REPORTHere, we report the case of an 82 year-old male patient with a history of cancer. In 2005 a prostatic adenocarcinoma was diagnosed (Gleason score 3 + 3 = 6) which was treated with radical prostatectomy (pT2c pN0 pMx). In the same year, a colic adenocarcinoma was diagnosed and he subsequently underwent a left hemicolectomy (pT3 pN0 pMx G2). During follow-up investigations, computed tomography (CT) scan showed the presence of a double neoplasm: a nodule of 12 mm in the right upper lobe (RUL) and a mass of 33 mm in the adipose tissue of the anterior mediastinum (Figure 1). Synchronized CT with 18-fluorodeoxyglucose-positron emission tomography (18-FDG-PET/CT) scan showed a maximum standardized uptake value (SUV max) of 3.9 and 6.3, respectively. The patient underwent Tru-Cut (Tc) -guided lung biopsy of the right upper lobe nodule. Histological examination reported multiple fragments of lung parenchyma at the site of adenocarcinoma (TTF1 +, CK7 +). A presurgical risk assessment was studied. Pneumological examination gave no contraindication for the surgical treatment. Arterial blood gases (ABG) were pH 7.39, pCO2 43.9 mmHg, pO2 76.2 mmHg, SpO2 95.7%, and HCO3− 26.4 mmol/l. Global spirometry examination yielded a postoperative FEV1 < 40% and therefore cardiopulmonary exercise testing (CPET) was indicated. It showed a nonsignificant reduction of myocardial oxygen consumption (81% of predictive value). This patients subsequently underwent a multidisciplinary evaluation that agreed upon surgical treatment.8

Computed tomography (CT) scans which show the (a) lung cancer; (b) thymic cancer and (c,d) the patient's last follow-up
The surgical procedure was performed with a uni-VATS approach through a right lateral thoracotomy of 4 cm at the fourth intercostal space between the middle and anterior axillary line. The patient underwent general anesthesia with a double lumen endotracheal tube to allow a selective ventilation of the left lung. First, we aimed to a carry out a segmentectomy in order to spare functional lung parenchyma. Unfortunately, there was diffuse emphysema replacement in the upper lobe and a RUL lobectomy was performed with dissection of the II, IV, VII, and VIII mediastinal node stations. In the second time, a thymectomy en bloc with the mediastinal adipose tissue was achieved. CO2 was not used and two 24 Fr chest drains were placed: the former in the pleural space inserted from the mini-thoracothomy access (Figure 2) and the latter in the mediastinal space, inserted anteriorly from the sixth right intercostal space. Operative time was about 200 min without significant blood loss. The specimens were sent to the pathology department for histological diagnosis.

Minithoracotomy and pleural drain in situ
These revealed that the nodule in the RUL was a lung adenocarcinoma with a papillary growth pattern of 60% and 40% acinar pattern, pT2a pN0 pMx G2, according to Travis WD et al.9
The mass in the mediastinal adipose tissue was a squamous cell thymic carcinoma. The immunohistochemistry found positivity for CK AE1-AE3, CD5, CD117, Pax-8, p63 and p40 (Figure 2) while TTF1, PSA, TdT was negative (Figure 3).

(a) Microphotographs of thymic carcinoma; (b) thymic carcinoma with immunohistochemistry for p40 and (c,d) lung adenocarcinoma
The postoperative course was regular, without any relevant air/liquid leak, pulmonary or cardiovascular complications. Postoperative ABG: pH 7.30, pCO2 71 mmHg, pO2 86 mmHg, SpO2 98.4%, and HCO3− 29.5 mmol/l. Chest drains were removed on the fourth (mediastinal) and eighth (pleural) postoperative day, because of prolonged liquid output. The hospital stay was nine days. After discharge, the patient underwent respiratory rehabilitation for one month. The patient later underwent an oncological follow-up with a CT thoracic scan and abdominal echography every 6 months (the last on May 2021 with no evidence of recurrence of malignancy).
DISCUSSIONThymic tumors have been associated with a high risk of developing simultaneous and/or metachronous extra-thymic tumors. Our patient is the embodiment of this evidence. Furthermore, previous studies have found that the most common association is with colorectal carcinoma, breast carcinoma, lung carcinoma, prostate carcinoma and leukemia/lymphoma10, 11 There are different theories for the rationale behind these associations.
First, in thymic carcinomas the most frequently mutated genes are TP53, missense mutation in the tumor suppressor CDKN2A or fibroblast growth factor receptor 3 (FGFR3) and FGFR3 amplification, or ALK translocation.12 These genes are commonly expressed in different tumors. Moreover, the thymus produces small lymphocytes (T cell) that play an important role in immunosurveillance, recognizing and destroying foreign cells. Thymic tumor development could start from an immune defect where thymic epithelium is unable to achieve T cell maturation. In this way, it increases the risk of neoplasia by an indirect process.13 Finally, autoimmunity can stimulate the proliferation of mutant clones of immunocompetent T cells that escape immunosurveillance and affect organs with an oncogenic effect.14
In the case reported here, after a multidisciplinary evaluation, we decided to proceed with single-stage surgery and a uni-VATS approach. This technique is largely used to perform various thoracic operations (pulmonary lobectomy, pulmonary atypical resection, excision of mediastinal masses, etc). Its widespread use is due to the reduction of postoperative complications and hospital stay, less postoperative pain, shorter permanence of chest tubes and better cosmetic results. It allows the excision of the whole neoplasia and dissection of the mediastinal nodes with oncological results not inferior to conventional thoracotomy or multiport VATS.15-18 The simultaneous excision of both the suspicious lesions aimed to ensure the correct oncological follow-up based on the pathological findings but we mainly wanted to avoid two-stage surgery that could mean a prolonged recovery after surgery because of the patient's age and comorbidities. The patient's clinical follow-up was characterized by two different exacerbations of congestive heart failure in October 2020 and January 2021. These events give strength to our previous surgical approach because two-stage surgery could have been delayed or been impossible to perform because of the occurrence of these clinical complications.
A review of the literature shows the lack of evidence and guidelines and literature reports are often limited to case reports or case series mainly because of low incidence of pulmonary nodules synchronous with mediastinal lesions.19 In addition, different surgical approaches are described (see Table 1). Deng et al. compared uniportal and multiportal VATS in two different cohorts (51 patients in total). They reported similar surgical and perioperative outcomes in the two groups (blood loss, time of operation, hospital and drainage stay).20 Zeng et al. recently analyzed the same outcomes in an eight patient case series, confirming uniportal VATS feasibility in concurrent pulmonary and mediastinal resections.21 Akar et al. described seven patients who underwent a combined lung resection and extended thymectomy with suxiphoid VATS in a two-year experience.22
TABLE 1. Studies focused on single-stage thoracic surgery Author N Lung resection Lung histology Mediastinal resection Mediastinal histology Surgical technique Type Lin et al.19 94 Wedge resection
5 Lobectomy
3 SCC
3 ADC
3 Other
2 Cyst excision
7 Thymectomy
3 Cyst
4 Thymoma
2 Thymic Hyperplasia
Three-port VATS Case series Deng et al.20 514 Wedge resection
2 Segmentectomy
27 Lobectomy
2 SCC
49 ADC
12 Cyst excision
39 Thymectomy
42 Cyst
9 Thymoma
18 three-port VATS
33 uni-VATS
Retrospective study Abu-Akar et al.22 73 Wedge resection
1 Segmentectomy
3 Lobectomy
1 SCC
5 ADC
1 Other
7 Thymectomy5 Cyst
2 Thymoma
Subxiphoid uni-VATS Case series Zeng et al.21 84 Wedge resection
2 Segmentectomy
2 Lobectomy
5 ADC
3 Other
3 Cyst excision
5 Thymectomy
6 Cyst
1 Thymoma
1 Other
Uni-VATS Case seriesSome studies have focused on the feasibility of a simultaneous bilateral surgical approach for lung cancer.23 They analyzed perioperative outcomes, medical costs and cancer recurrence in patients with bilateral multiple primary lung cancers (MPLC) making comparison with a control group of patients who underwent two-stage surgery. A concurrent surgical approach yielded a disease-free survival significantly higher than staged resections (67.7 vs. 45.9% at 5 years). Simultaneous resection resulted in a significant advantage in reducing the costs. Anyway, both these experiences applied two different incisions to excise both cancers.24
To the best of our knowledge there are no studies in the literature which report if simultaneous resections with a single incision using the uni-VATS technique may enable a reduction in medical costs and be oncologically reliable in patients with lung and mediastinal tumors.
In conclusion, here we report the case of a patient in which there was an unusual association of different tumors that may have been caused by thymic carcinoma characteristics. On the other hand, we also wanted to highlight the versatility of the uni-VATS approach which allows management of challenging clinical and oncological situations. Avoiding two-stage surgery may be a very useful way to reduce hospitalization costs without affecting oncological radicality but more studies are needed to focus on this matter.
ACKNOWLEDGMENTSNo support or funding.
CONFLICT OF INTERESTThe authors report no conflict of interest.
REFERENCES
1Travis WD, Brambilla E, Burke AP, Marx A, Nicholson AG. WHO classification of tumors of the lung, pleura, thymus and heart. IARC Press: Lyon; 2015. 2Filosso PL, Yao X, Ruffini E, Ahmad U, Antonicelli A, Huang J, et al. Comparison of outcomes between neuroendocrine thymic tumours and other subtypes of thymic carcinomas: a joint analysis of the European Society of Thoracic Surgeons and the International Thymic Malignancy Interest Group. Eur J Cardiothorac Surg. 2016; 50(4): 766– 71. 3Yen YT, Lai WW, Wu MH, Lin MY, Chang JM, Hsu IL, et al. Thymic neuroendocrine carcinoma and thymoma are both associated with increased risk of extrathymic malignancy: a 20-year review of a single institution. Ann Thorac Surg. 2011; 91(1): 219– 25. 4Yanagiya M, Matsumoto J, Kawahara T, Yamaguchi H, Nagayama K, Anraku M, et al. Influence of smoking and histologic subtype on developing extrathymic malignancy in thymoma patients. Ann Thorac Surg. 2019; 107(5): 1532– 9. 5Shigemura N, Akashi A, Funaki S, Nakagiri T, Inoue M, Sawabata N, et al. Long-term outcomes after a variety of video-assisted thoracoscopic lobectomy approaches for clinical stage IA lung cancer: a multi-institutional study. J Thorac Cardiovasc Surg. 2006; 132(3): 507– 12. 6Yan TD, Black D, Bannon PG, McCaughan BC. Systematic review and meta-analysis of randomized and nonrandomized trials on safety and efficacy of video-assisted thoracic surgery lobectomy for early-stage non-small-cell lung cancer. J Clin Oncol. 2009; 27(15): 2553– 62. 7Kaseda S, Aoki T, Hangai N, Shimizu K. Better pulmonary function and prognosis with video-assisted thoracic surgery than with thoracotomy. Ann Thorac Surg. 2000; 70(5): 1644– 6. 8Frasca L, Longo F, Tacchi G, Stilo F, Zito A, Brunetti B, et al. Importance of muldisciplinary management of giant mediastinal sarcoma: a case report with phrenic nerve reconstruction. Thorac Cancer. 2020; 11(6): 1734– 7. 9Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger KR, Yatabe Y, et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol. 2011; 6(2): 244– 85. 10Hamaji M, Sozu T, Machida R, Watanabe SI, Yoshida K, Toyooka S, et al. Mortality from extrathymic malignancy after thymic tumour resections: incidences and risk factors. Interact Cardiovasc Thorac Surg. 2019; 29(5): 729– 36. 11Weksler B, Nason KS, Mackey D, Gallagher A, Pennathur A. Thymomas and extrathymic cancers. Ann Thorac Surg. 2012; 93(3): 884– 8. 12Enkner F, Pichlhöfer B, Zaharie AT, Krunic M, Holper TM, Janik S, et al. Molecular profiling of thymoma and thymic carcinoma: genetic differences and potential novel therapeutic targets. Pathol Oncol Res. 2017; 23(3): 551– 64. 13Souadjian JV, Enriquez P, Silverstein MN, Pépin JM. The spectrum of diseases associated with thymoma. Coincidence or syndrome? Arch Intern Med. 1974; 134(2): 374– 9. 14Papatestas AE, Osserman KE, Kark AE. The relationship between thymus and oncogenesis. A study of the incidence of non thymic malignancy in myasthenia gravis. Br J Cancer. 1971; 25(4): 635– 45. 15Hirai K, Takeuchi S, Usuda J. Single-incision thoracoscopic surgery and conventional video-assisted thoracoscopic surgery: a retrospective comparative study of perioperative clinical outcomesdagger. Eur J Cardiothorac Surg. 2016; 49(Suppl 1): i37– 41. 16Zhu Y, Liang M, Wu W, Zheng J, Zheng W, Guo Z, et al. Preliminary results of single-port versus triple-port complete thoracoscopic lobectomy for non-small cell lung cancer. Ann Transl Med. 2015; 3(7): 92. 17Bourdages-Pageau E, Vieira A, Lacasse Y, Figueroa PU. Outcomes of uniportal vs multiportal video-assisted thoracoscopic lobectomy. Semin Thorac Cardiovasc Surg. 2020; 32(1): 145– 51. 18Harris CG, James RS, Tian DH, Yan TD, Doyle MP, Gonzalez-Rivas D, et al. Systematic review and meta-analysis of uniportal versus multiportal video-assisted thoracoscopic lobectomy for lung cancer. Ann Cardiothorac Surg. 2016; 5(2): 76– 84. 19Lin F, Xiao Z, Mei J, Liu C, Pu Q, Ma L, et al. Simultaneous thoracoscopic resection for coexisting pulmonary and thymic lesions. J Thorac Dis. 2015; 7(9): 1637– 42. 20Deng J, She Y, Zhao M, Ren Y, Zhang L, Su H, et al. Simultaneously thoracoscopic resection of lung cancer and anterior mediastinal lesions by video-assisted thoracoscopic surgery. Ann Transl Med. 2019; 7(14): 333. 21Zeng L, Zhuang R, Tu Z. Simultaneous uniportal video-assisted thoracic surgery for pulmonary nodules and synchronous mediastinal lesions. Wideochir Inne Tech Maloinwazyjne. 2021; 16(2): 390– 6. 22Abu-Akar F, Gonzalez-Rivas D, Yang C, Lin L, Wu L, Jiang L. Subxiphoid uniportal VATS for thymic and combined mediastinal and pulmonary resections - a two-year experience. Semin Thorac Cardiovasc Surg. 2019; 31(3): 614– 9. 23Zhang Y, Wang Y, Lv C, Shu X, Wang J, Yang Q, et al. Clinical analysis of 56 cases of simultaneous bilateral video-assisted thoracoscopic surgery for bilateral synchronous multiple primary lung adenocarcinoma. J Thorac Dis. 2018; 10(12): 6452– 7. 24Zheng H, Peng Q, Xie D, Duan L, Zhao D, Jiang G, et al. Simultaneous bilateral thoracoscopic lobectomy for synchronous bilateral multiple primary lung cancer-single center experience. J Thorac Dis. 2021; 13(3): 1717– 27.
Comments (0)