
Remember me







Neuroblastoma, an embryonal tumor arising from the sympathetic nervous system, is the most common neonatal malignancy that accounts for >20% of neonatal cancers[1]. The most common location for neuroblastoma to originate (i.e., the primary tumor) is on the adrenal glands but primary cancer originating from lung is very rare. We report a case of newborn who was referred to us as case of persistent pneumonia but was diagnosed as primary congenital neuroblastoma of lung.
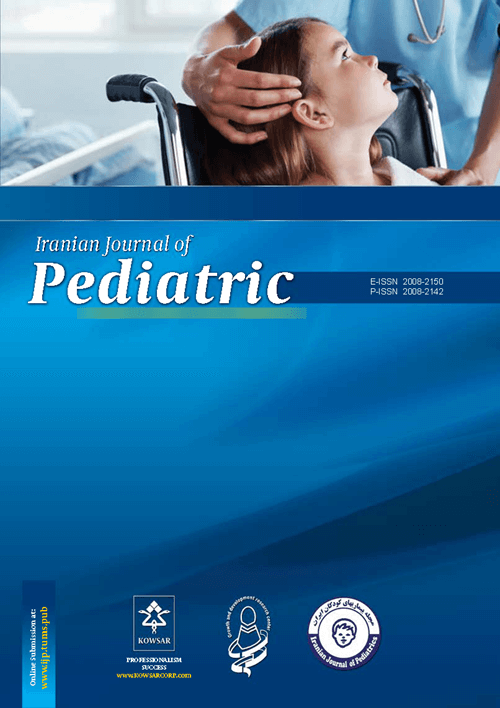
Baby Y, female infant was referred at age of 23 days with difficulty in breathing from age of 13 days. The infant was born by normal vaginal delivery with weight of 2.6 kg and Apgar of 7/8/8. Ante-natal period was uncomplicated with normal scans. Infant had fever (101ËÂ to 102ËÂ F) on and off from 13 days of age and respiratory distress for which baby was admitted in hospital. Baby received injectable antibiotics in referral NICU for 10 days. Baby was referred to us in view of persistence of respiratory distress and X-ray findings. At admission, the infant weighed 2.5 kg, had a temperature of 37.5oC, HR 148/min, RR 50/min, BP 64/42 mm Hg, mild to moderate subcostal and intercostal retractions, air entry decreased on right side, dusky peripheries, SpO2 65% on room air, SpO2 93% with oxygen by hood with flow of 5 liters/min, liver 2cm below costal margin, spleen 1cm below costal margin, pedal edema. Blood counts revealed neutrophilic leukocytosis (total count 18600/mm3, neutrophils 66%), C-reactive protein -41.4 mg/l. Chest X-ray showed right upper lobe heterogeneous opacity and distal consolidation with right lower lobe showing patchy consolidation (Fig. 1).
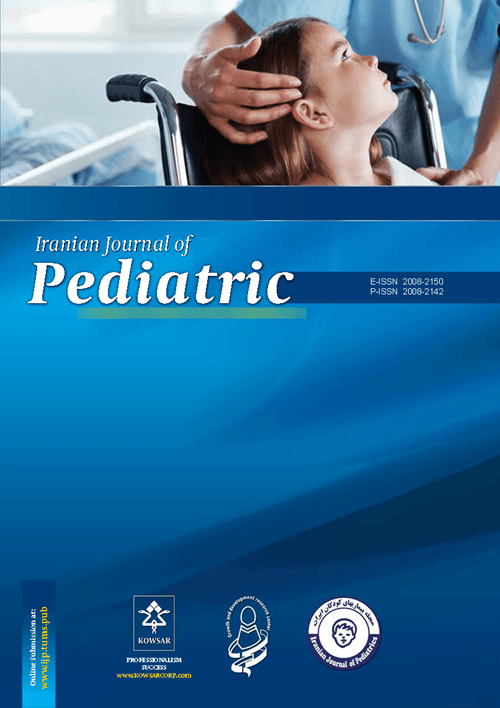
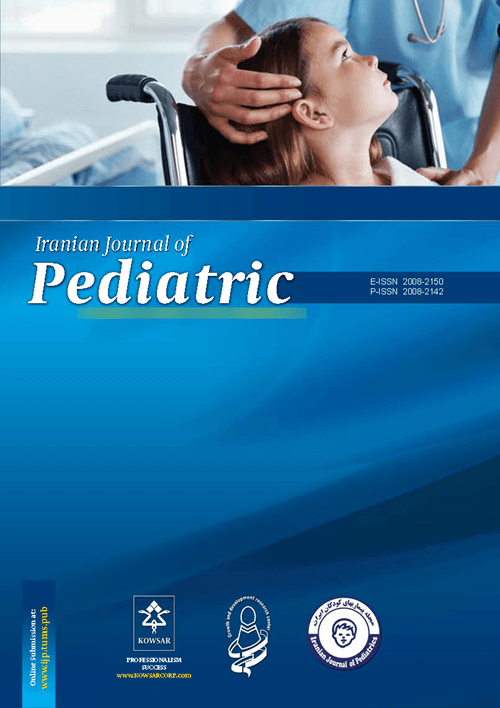
Ultrasonography showed hepato¬splenomegaly in abdomen and in chest showing intrathoracic soft tissue mass lesion in right paratracheal and upper lobe with distal consolidation of middle and lower lobe. The infant was started on intravenous antibiotics and supportive care. In view of persistence of respiratory distress repeat X- ray was done after 1 week which didn’t show any improvement (Fig. 2). Chest CT scan showed posterior and apical segments of right upper lobe having consolidation without air bronchogram with small central cavitation. Anterior segments of right upper lobe and right middle lobe lateral segment showed nodular lesions. Right lower lobe basal segments showed areas of consolidation with curvilinear air lucencies with intercavitory bodies. Left lower lobe showed multiple confluencing nodular lesions with curvilinear air lucencies (Fig 3). CECT chest showed possibility of metastatic neuroblastoma and Fine needle aspiration cytology (FNAC) and biopsy was planned. FNAC was done which revealed moderate cellular cells which were mostly acute inflammatory cells with atypical tumor cells. Individual cells were round to polygonal cells having scanty to moderate amount of eosinophilic cytoplasm with anisopoikilocytosis with hyperchromasia, high nuclear to cytoplasmic ratio with prominent nucleoli. Biopsy showed small, round, blue cell tumor cells with high nuclear to cytoplasmic ratio and presence of Homer-Wright pseudo rosettes. Baby was started on chemo¬therapy but infant succumbed to death after 10 days of starting treatment.
Congenital neuroblastoma is defined as neuro-blastoma identified within a month of birth[1]. Neuroblastoma is slightly more common in boys than in girls with a male to female sex ratio of 1.2:1[2]. Neuroblastoma is especially unique because of its varied presentation in the young. The tumor has been detected as an unexpected finding in the fetus either as a cystic or solid mass above upper pole of the kidney[3,4].
Neuroblastoma is characterized with densely cellular, primitive, “small blue-cell tumor” appearance. Undifferentiated neuroblastoma may 
Fig. 1: Chest X-ray at admission

Fig. 2: Chest X-ray after treatment for 1 week
Fig. 3: Multiple confluencing nodular lesions with curvilinear air lucencies in Chest CT scan
be difficult to distinguish by electron microscopy from other small-cell malignant tumors. The predominance of blue staining is due to the fact that the cells consist predominantly of nucleus, thus they have scant cytoplasm[5]. The tumor cells are reactive for neuron specific enolase (NSE), synaptophysin, neurofilament, and focally positive for S-100 protein and they stain negative for desmin, actin, leukocyte common antigen, cytokeratin, and the Ewing antigen[6]. Urinary catecholamines are raised in >90% of neuroblastomas but only in 33% of perinatal neuroblastomas. I131 or I123 (preferred) meta-iodo benzyl guanidine (MIBG) scintigraphy is highly sensitive and specific. The treatment of neuroblastoma depends on the stage, and it includes surgical excision, multiagent chemotherapy, and bone marrow transplan-tation[7].
Comments (0)