
Remember me









Eosinophilic granulomatosis with polyangiitis (EGPA) is an autoimmune disease characterized by small-to-medium-sized vessel necrotizing vasculitis, asthma and blood and tissue eosinophilia.1-4 Anti-neutrophil cytoplasmic antibodies (ANCA) are positive in approximately 30%–40% of these patients.4-6 Patients positive for ANCA more commonly had neurological and renal involvement compared with patients negative for ANCA, who had more cardiac and lung manifestations.4-6 The treatment of relapsing EGPA is challenging due to the lack of a consensus on its optimal management.7 The efficacy of some biologics, such as omalizumab, mepolizumab, benralizumab and rituximab, has been evaluated in these patients,8-11 but no single agent can ensure a complete control of this disease and the comparative efficacy remains unclear. Here, we report the clinical benefits after switching from omalizumab to mepolizumab in an ANCA-negative EGPA patient on her abdominal and cutaneous manifestations.
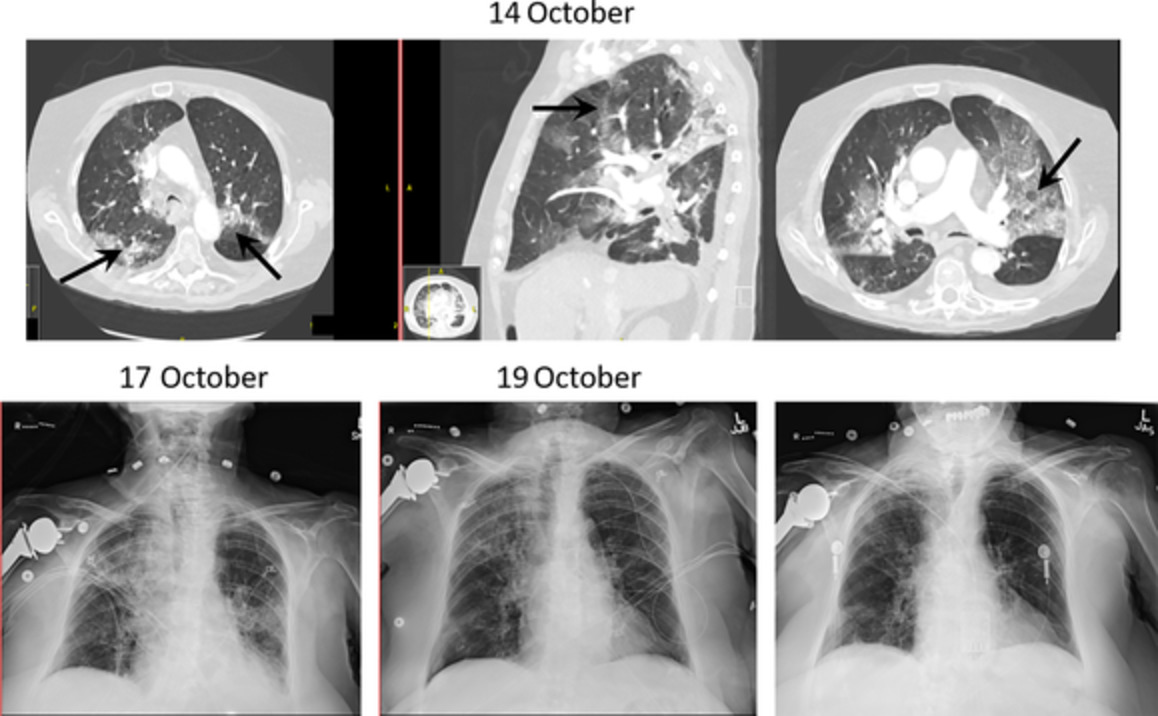
CASE REPORTA 24-year-old woman presented to our outpatient clinic with a recurrent cough, wheezing, skin rash, abdominal pain and diarrhoea. During the 3 years before her first visit to our hospital, she had been admitted to another local hospital several times due to these symptoms, but no definite diagnosis was established there. Also, her asthma became uncontrolled despite treatment with a fixed high-dose inhaled corticosteroid and long-acting beta2 agonists. In that hospital, hypereosinophilia was also observed, with the highest blood eosinophil count of 8480/μl, and the pathology of her skin biopsy showed vasculitis with infiltration of eosinophils. During one episode of hospitalization, she developed cough and dyspnoea again and the high-resolution computed tomography (HRCT) of the chest revealed peripheral ground-glass opacification and consolidations at bilateral upper lobes and more at the right upper lobe (Figure 1A1–A3), which were refractory to antibiotic therapy but finally resolved on the chest radiograph after administration of intravenous methylprednisolone at 40 mg every 8 h for 5 days with gradual tapering. After hospital discharge, a maintenance prednisolone at 5–10 mg per day was required to control her asthma and extra-pulmonary symptoms. Her past history was notable for a diagnosis of allergic asthma at a local clinic since early childhood.

Axial and coronal views of the chest computed tomography during flare-up (A1–A3) and remission (B1–B3) of eosinophilic granulomatosis with polyangiitis
In our hospital, all autoimmune profiles were negative. The allergen panel was positive for dust mites. The level of serum total immunoglobulin-E (IgE) was 247 IU/ml. Results of the pulmonary function test were normal when her asthma was stable, but wide variations of her peak expiratory flow rate (PEFR) were observed during follow-up (Figure 2). ANCA-negative EGPA was diagnosed and the initial Birmingham Vasculitis Activity Score (BVAS) was 14. Despite add-on therapies including montelukast and inhaled tiotropium, her Asthma Control Test (ACT) scores were still below 20. Subcutaneous omalizumab 300 mg was administered every 4 weeks initially, because no other biologics were available for severe asthma at that time. Her asthma control became better thereafter, with reduced frequency of coughing and chest tightness, and significant improvements in ACT scores and PEFR (Figure 2). Unfortunately, she developed another relapse of her abdominal and skin manifestations, requiring hospitalization to her previous hospital where the abdominal CT revealed diffuse wall thickening over the colon and small amount of ascites. The dose of her maintenance prednisolone increased to 10-20 mg per day after discharge. In addition, her biologic was switched to mepolizumab at an initial dose of 100 mg per month, when this agent was available for the treatment of severe eosinophilic asthma in our hospital (Table 1). Her hypereosinophilia and extra-pulmonary symptoms significantly improved thereafter, and the dose of her maintenance corticosteroid could be reduced (Figure 2). The monthly dose of mepolizumab was increased to 300 mg 10 months later, when this agent was approved for EGPA in our country. At this higher dose of mepolizumab, her extra-pulmonary symptoms nearly disappeared, and the dose of daily prednisolone could be gradually tapered off (Table 1 and Figure 2). The chest HRCT performed when she was in remission revealed total resolution of previous lung infiltrates (Figure 1B1–B3).

Time course of blood eosinophil counts, treatments and clinical parameters. *Month 0: Initial visit to our hospital. ACT, Asthma Control Test; BVAS, Birmingham Vasculitis Activity Score; PEFR, peak expiratory flow rate
TABLE 1. Summary of blood eosinophil counts, events and treatment highlights Time (months) Eosinophil percentage (%) Eosinophil count (/μl) Event/setting Treatment highlights −15 53 8480 Hospitalization (diarrhoea, skin rash, asthma exacerbation) IV methylprednisolone −3 41.3 2480 Hospitalization (asthma exacerbation, pulmonary infiltrates) IV methylprednisolone 0 7.6 550 Initial visit to our hospital (outpatient clinic) Add montelukast and inhaled tiotropium 7 35.9 2731 Outpatient clinic Initiation of SC omalizumab 300 mg/month 10 22.3 2332 Hospitalization (generalized painful skin rash) IV methylprednisolone 11 10.7 542 Hospitalization (abdominal pain, diarrhoea) IV methylprednisolone 12 17.1 2927 Outpatient clinic Switching to SC mepolizumab 100 mg/month 16 0.9 51 Outpatient clinic SC mepolizumab 100 mg/month 23 NA NA Outpatient clinic Increasing SC mepolizumab dose to 300 mg/month 27 0.3 11 Outpatient clinic SC mepolizumab 300 mg/month Abbreviations: IV, intravenous; NA, not available; SC, subcutaneous. DISCUSSIONIn this report, we describe a case of relapsing EGPA, where the use of mepolizumab demonstrated superior efficacy over omalizumab in her abdominal and cutaneous vasculitis symptoms. To our knowledge, few previous studies have addressed the relative therapeutic benefits between anti-IgE and anti-interleukin (IL)-5 biologics in EGPA.12
In our case, the use of omalizumab improved her asthma control but was ineffective for the extra-pulmonary symptoms. In EGPA patients, omalizumab was reported to reduce the daily corticosteroid requirement and the frequency of asthma exacerbation.8, 13 Clinical studies of omalizumab in EGPA, however, are still limited and its benefits are controversial.14-17 Furthermore, some case reports even implied an increased risk for the development of EGPA among asthmatic patients treated with omalizumab, probably related to the reduction in steroid dosage.17-19 Therefore, clinical use of this agent remains a concern in these patients.
The management of extra-thoracic manifestations of EGPA is challenging due to its complex immunopathogenesis involving both eosinophilic proliferation and ANCA-associated vasculitis, which are the main effectors of organ damage and the hallmarks of the disease.6, 20, 21 IL-5, IL-4 and IL-13, which are responsible for eosinophil activation and tissue recruitment, are overexpressed and contribute to Th2-mediated response.20-22 On the other hand, the association between eosinophilic inflammation and ANCA positivity remains unclear, and biomarkers capable of monitoring disease activity or predicting treatment response in these patients are still lacking.8, 23
The efficacy of mepolizumab for relapsing or refractory EGPA has been demonstrated by its phase 3 trial (MIRRA).9 The study population in that trial, however, was mainly ANCA-negative and 43% of participants in the mepolizumab arm still developed vasculitis relapses, despite a remarkable reduction in blood eosinophil count.9 Furthermore, 47% of those in the mepolizumab group did not have protocol-defined remission.9 The superior benefits of mepolizumab over omalizumab in our case were not surprising and compatible with the results reported by Canzian et al., but differences between these two biologics on extra-pulmonary manifestations of EGPA were not described in that study.12
The approved dose of mepolizumab for EGPA is 300 mg every 4 weeks.9 In our patient, mepolizumab was initially administered at a lower dose approved for severe eosinophilic asthma due to regulatory issue in our country. In a study of 18 EGPA patients with severe asthma but without active vasculitis, Vultaggio et al. reported that mepolizumab administered at 100 mg per month provided clinically relevant benefits in asthma control and the requirements of corticosteroids and other immunosuppressants.24 Another study conducted by Canzian et al. revealed similar remission rates at 12 months among patients receiving monthly mepolizumab at 100 and 300 mg (76% and 82%, respectively), which was also consistent with the results from an European multicentre observational cohort.12, 25 Nonetheless, it is concerning that a low-dose mepolizumab may increase the relapse of asthma in EGPA patients.26 The better steroid-sparing effect observed in our case also supports the use of a high-dose mepolizumab in these patients.
The benefits of mepolizumab in our patient reported here may be fragile, since the long-term outcomes are yet unclear. No previous studies have been conducted to compare the relative efficacy of different biologics targeting IL-5 in EGPA. Recently, Menzella et al. described remarkable improvements in asthma and ear–nose–throat symptoms in an EGPA patient after switching from mepolizumab to benralizumab, which was also consistent with the results reported by Bormioli et al.27, 28 These might result from a better ability of benralizumab to reduce the number of eosinophils in various tissues by 90%–100%.10, 27 Moreover, some studies suggest that concurrent use of mepolizumab and rituximab may be more beneficial for the treatment of ANCA-positive EGPA patients.11, 29, 30 Therefore, the relative efficacy of biologics in each patient may be influenced by the multiple and different mechanisms involved.30
In conclusion, EGPA is a heterogeneous disease involving different mechanisms, and the optimal treatment strategies for these patients remain unclear. Experience from our case suggests that switching to an anti-IL-5 biologic may be considered in EGPA patients having an incomplete or poor response to omalizumab. Our results may also provide insights into the complex interaction between eosinophilic inflammation and vasculitis in these patients. Further studies are required to investigate the relative therapeutic benefits between different biologics and the role of precision medicine in EGPA.
AUTHOR CONTRIBUTIONPing-Hung Kuo provided conception and design of the article. Yu-Hsuan Chen drafted the first version of the manuscript. Ping-Hung Kuo provided professional advice and revised the manuscript, and both authors agreed for the final version of the manuscript.
ETHICS STATEMENTThe authors declare that appropriate written informed consent was obtained for the publication of this manuscript and accompanying images.
Comments (0)