An autopsy case report of neuronal intermediate filament inclusion disease presenting with predominantly upper motor neuron features
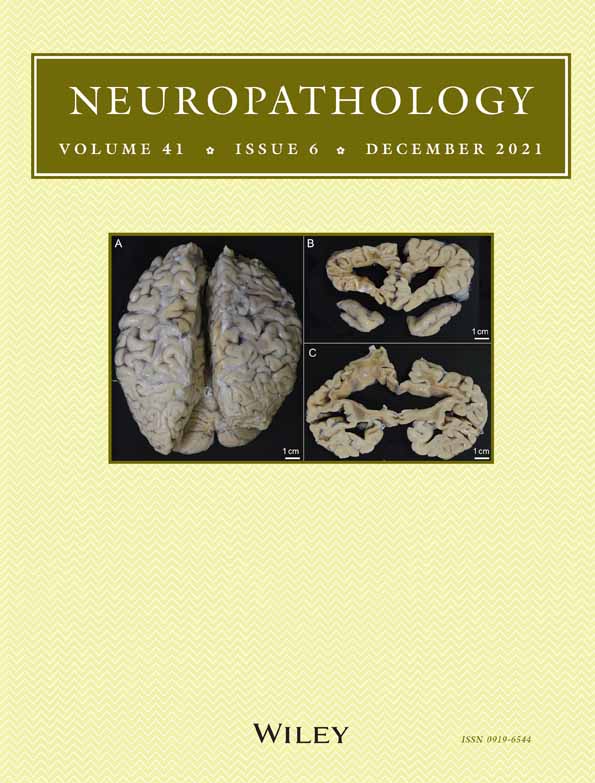
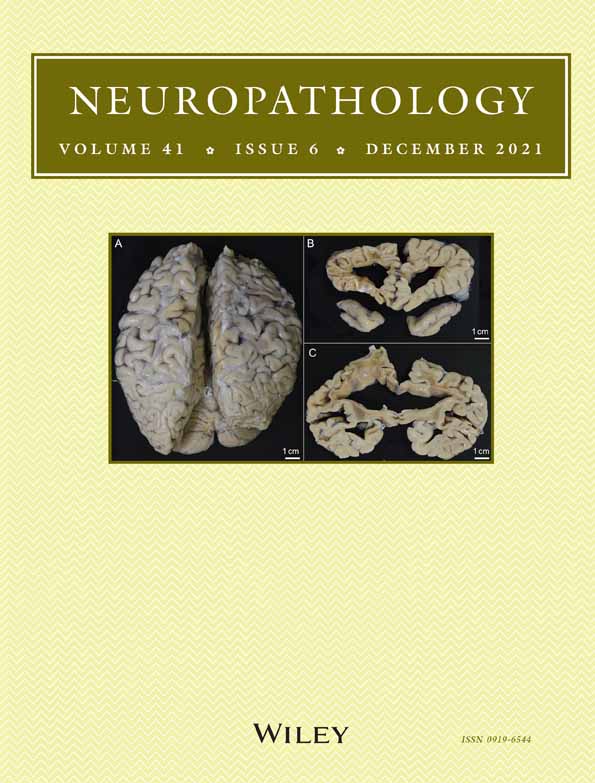
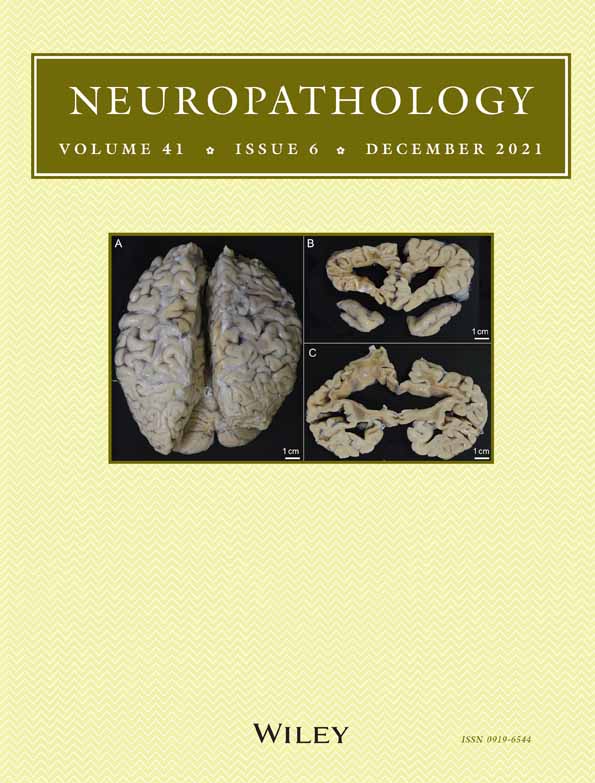
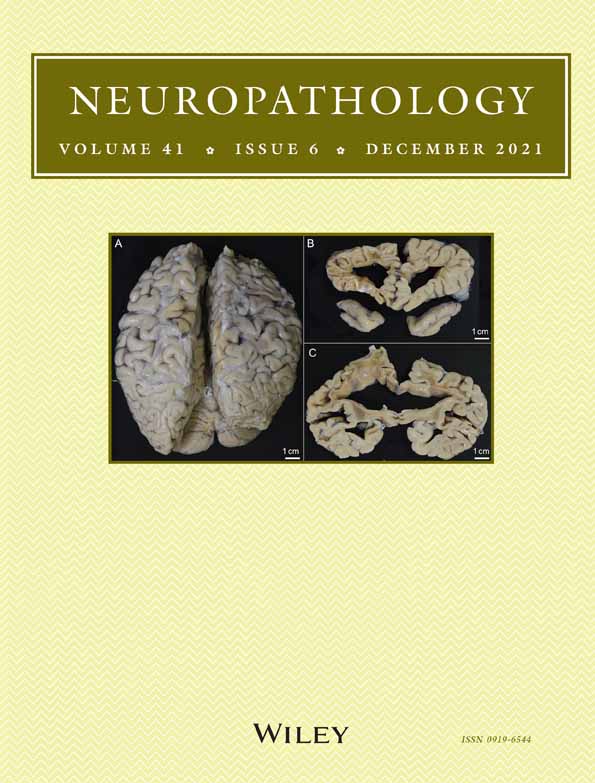
We describe an autopsy case of neuronal intermediate filament inclusion disease (NIFID), a subtype of frontotemporal lobar degeneration (FTLD) with the appearance of fused-in-sarcoma (FUS) inclusions (FTLD-FUS). A 57-year-old man developed dysarthria and dysphagia. One year and five months later, he was admitted to a hospital, and pseudobulbar palsy and right upper motor neuron signs were observed on examination. Needle electromyography revealed no active or chronic denervation. His neurological symptoms gradually deteriorated, and behavioral alterations occurred. He died of hemoperitoneum secondary to rupture of a ureteric tumor. The total duration of the disease was six years and 10 months. Neuropathologically, the frontal cortex, including the motor cortex, and the pyramidal tract were severely affected, whereas the lower motor neurons in the spinal cord and brainstem were mildly damaged. The striatum and substantia nigra were also severely damaged. Hyaline conglomerate inclusions, neuronal cytoplasmic inclusions with a distinct eosinophilic core (so-called cherry spot), Pick body-like inclusions, and eosinophilic round inclusions were observed in the remaining neurons. Immunohistochemical examination revealed that these inclusions were immunoreactive for FUS. HC inclusions were also immunoreactive for α-internexin and phosphorylated neurofilament protein. FUS-immunoreactive NCIs were abundant in the basal ganglia but not in the hippocampus, in contrast to previously reported NIFID cases. Furthermore, Bunina bodies identified by immunohistochemistry for cystatin C were also observed in the lower motor neurons. Bunina bodies may be present in NIFID. This case confirms the pathological heterogeneity of NIFID and supports the notion of the difference between amyotrophic lateral sclerosis and NIFID.




Comments (0)