
Remember me

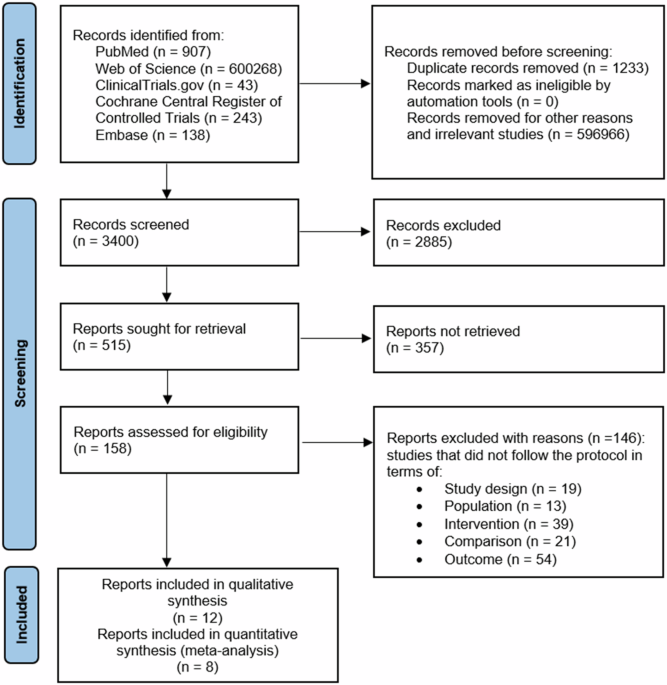

A total of 2506 patients met the inclusion criteria and were prescribed ICS/LABA medication for ≥3 months in Canada (123/2,506 [4.9%]), China (321/2,506 [12.8%]), Europe (1,364/2,506 [54.4%]), Japan (273/2,506 [10.9%]), and the US (425/2,506 [17.0%]) (Supplementary Fig. 1). When stratified by subpopulations, most ICS/LABA users were prescribed ICS/LABA as maintenance-only therapy in all 5 regions (Canada, 74/123 [60.2%]; China, 237/321 [73.8%]; Europe, 747/1,364 [54.8%]; Japan, 211/273 [77.3%]; and the US, 333/425 [78.4%]) (Fig. 2). Among ICS/LABA MART users, patients in Canada, China, Europe, and Japan were predominantly prescribed ICS/formoterol as MART as recommended by GINA; in contrast, most patients in the US were prescribed an ICS/LABA therapy not recommended for MART by GINA (i.e., non-ICS/formoterol combinations) (Supplementary Fig. 1).
Fig. 2: ICS/LABA prescription by region.
ICS inhaled corticosteroid, LABA long-acting β2-agonist, MART maintenance and reliever therapy, SABA short-acting β2-agonist, US United States.
Patient demographics and clinical characteristicsFor ICS/LABA users across all regions, mean (SD) age ranged from 43.4 (16.4) to 53.0 (17.5) years, most patients were female (51.7–55.4%), and most had never smoked (58.2–76.6%) (Table 1). In all five regions, the mean Charlson Comorbidity Index (CCI) score was 0.1 (SD range: 0.4–0.5). Allergic rhinitis was the most common comorbidity in China (50.8%), Europe (39.9%), and the US (52.2%), while hypertension was the most common comorbidity in Canada (23.6%) and Japan (23.1%) (Table 1). Most patients were in GINA treatment Step 4 in each region, with China having the lowest proportion of patients in GINA treatment Step 5 (0.3%) (Table 2).
Table 1 Patient demographics at baseline for all ICS/LABA users.Table 2 Clinical characteristics and exacerbations at baseline for all ICS/LABA users.Concomitant medications and treatment adherenceAcross all regions, ICS/LABA users were most commonly prescribed a medium total daily dose of ICS (40.5–54.6%), while high total daily doses of ICS were more commonly prescribed among ICS/LABA maintenance users versus MART users in all regions except China (Supplementary Table 1).
The most commonly co-prescribed asthma medication for all ICS/LABA users in Canada, Europe, and the US was SABA (61.8%, 45.0%, and 67.8%, respectively) (Supplementary Table 1). Co-prescription of SABA was consistently higher among ICS/LABA maintenance versus MART users, except in Japan, where SABA prescription was similar between maintenance and MART users (Fig. 2). For all ICS/LABA users in Japan, leukotriene receptor antagonist (LTRA) prescriptions were most common (32.6%), while in China, long-acting muscarinic antagonists (LAMA) were the most frequently co-prescribed medication (45.6%) (Supplementary Table 1). When stratified by MART and maintenance subpopulations, in Japan, LTRA and LAMA were more commonly co-prescribed among ICS/LABA MART users (40.4% and 10.5%, respectively) than maintenance users (30.8% and 5.7%, respectively), while oral corticosteroids (OCS) were more commonly co-prescribed in maintenance versus MART users (5.2% vs. 3.5%) (Supplementary Table 1). In China, ICS/LABA maintenance users were more likely to receive LAMA (49.2%) or LTRA (18.1%) than MART users (40.4% and 8.5%, respectively) (Supplementary Table 1).
In Canada, Europe, Japan and the US, >90% of all ICS/LABA users were reported as being moderately–completely adherent to their currently prescribed asthma treatment by their treating physician, while in China, most patients were reported as moderately (40.0%) or very adherent (47.2%) (Supplementary Table 1). When stratified by subpopulation, the proportion of patients classed as moderately–completely adherent was broadly similar between ICS/LABA maintenance and MART users in all regions, though there was some variation between subpopulations (Supplementary Table 1).
Prescribing patterns and physicians’ reasons for treatment choiceIn Canada, Europe, Japan, and the US, treating physicians were most commonly PCPs, followed by pulmonologist/respiratory specialists; allergists made up the smallest proportion of specialists sampled. In China, all physicians were hospital-based specialists (Table 1).
For all ICS/LABA users, the most common reasons physicians gave for their choice of currently prescribed ICS/LABA treatment was to provide sustained 24-hour symptom relief and improve shortness of breath in Canada (57.7%, 58.4%), Europe (60.8%, 57.9%), and Japan (57.9%, 40.3%). In China, improvement in daytime symptomatic relief was prioritized together with improvements in shortness of breath (91.6%, 64.5%), while in the US, sustained 24-hour symptom relief and improvement in daytime symptomatic relief were prioritized (68.2%, 63.3%). When stratified by subpopulation, the key reasons for ICS/LABA MART prescriptions were immediate onset of action in Canada (62.5%) and Europe (60.7%), improvement in daytime symptomatic relief in China (86.5%), improvement in shortness of breath in Japan (54.4%) and sustained 24-hour symptom relief in the US (78.8%). The main reason for ICS/LABA maintenance-only prescriptions was sustained 24-hour symptom relief in Canada (62.2%), Europe (63.3%), Japan (62.1%), and the US (66.1%), whereas improvement in daytime symptomatic relief remained the main reason in China (91.6%).
Clinical burdenBased on available data, the mean (SD) pre-bronchodilator FEV1 % predicted was highest among all ICS/LABA users in Canada (91.2 [109.0]) compared with all other regions. China had the lowest mean (SD) number of exacerbations of any severity (0.2 [0.6]) and exacerbations resulting in an OCS course and/or ER visit and/or hospitalization in the last 12 months (0.1 [0.4]), compared with all other regions (Table 2). The mean (SD) number of exacerbations of any severity in the last 12 months was greater among ICS/LABA MART users versus maintenance users in Canada, Europe, Japan, and the US (Canada: 1.0 [1.2] vs. 0.8 [1.7]; Europe: 0.8 [1.2] vs. 0.7 [1.2]; Japan: 0.7 [1.4] vs. 0.4 [1.2]; US: 1.0 [2.0] vs. 0.8 [1.2]), but remained similar in China (China: 0.2 [0.6] vs. 0.2 [0.6]).
Physician-reported SABA use varied between regions (Fig. 3). The proportion of patients with any SABA use was considerably higher in Canada (69.1%), Europe (61.3%), and the US (77.2%) compared with China (24.1%) and Japan (30.8%); most patients in China and Japan received no SABA or did not use their prescribed SABA. Everyday use was low throughout all regions, ranging from 0.6%–6.5%. When stratified by subpopulation, the proportion of patients with any SABA use was higher among ICS/LABA maintenance versus MART users in Canada (70.3% vs. 66.7%), Europe (66.3% vs. 54.1%) and the US (78.1% vs 74.1%), but was higher among MART versus maintenance users in China (27.0% vs. 25.7%) and Japan (33.3% vs. 29.4%).
Fig. 3: Physician-reported short-acting reliever medication use.
ICS inhaled corticosteroid, LABA long-acting β2-agonist, MART maintenance and reliever therapy, US United States.
Economic burdenHealthcare resource utilizationICS/LABA users in Japan had the highest mean (SD) number of unscheduled HCP visits (9.6 [4.9]), whereas China (3.1 [2.7]), Europe (2.4 [1.9]), and the US (2.3 [2.1]) had the highest number of scheduled HCP visits compared with other regions (Table 3). A higher mean (SD) number of hospitalizations due to asthma were reported in Europe and the US (each 0.3 [0.7]) compared with Canada (0.1 [0.5]), China (0.1 [0.4]), and Japan (0.1 [0.5]) (Table 3). There were no differences in HCRU between those receiving ICS/LABA as MART or as maintenance in any region (Table 3).
Table 3 HCRU in the last 12 months for all ICS/LABA users and MART and maintenance subpopulations.Work and activity impairmentAmong all ICS/LABA users with available data, the proportion of patients in full-time employment at baseline ranged from 67.0% to 42.9% across all regions (Table 1). In the China, Europe, and US regions, mean percentage (SD) overall work impairment ranged from 39.8% (21.3) to 17.4% (17.8), with absenteeism ranging from 8.8% (9.1) to 2.5% (11.6) (Fig. 4).
Fig. 4: WPAI of all ICS/LABA users.
a China, b Europe, and c the US. Data for Canada and Japan were not collected. ICS inhaled corticosteroid, LABA long-acting β2-agonist, SD standard deviation, US United States, WPAI Work Productivity and Activity Impairment.
Humanistic burdenSymptom burdenICS/LABA users in Canada and the US had the highest mean (SD) number of physician-reported symptom-free days in the past 30 days (20.6 [8.9] and 19.7 [8.6], respectively). Similar results were observed for patient-reported symptom-free days in China, Europe, Japan, and the US (Table 4). The most troublesome symptoms among all ICS/LABA users varied across regions, and included shortness of breath when exposed to a trigger (Canada [20.3%]), productive cough (China [28.0%] and Japan [18.0%]), and shortness of breath during exertion (Europe [33.4%] and the US [35.5%]) (Table 4).
Table 4 Symptom burden for all ICS/LABA users.Health-related quality of lifeAmong patients with available data in Europe and the US, approximately 1 in 3 patients in all subpopulations reported having not well-controlled asthma (Europe: 31.5–34.6%; US: 30.9–35.1%) (Supplementary Fig. 2A). The impact of asthma on sleep was also similar across all subpopulations, with mean JSEQ scores ranging from 3.0–3.4 in Europe and 2.9–3.6 in the US (Supplementary Fig. 2B). When stratified by asthma control status, mean EQ-5D utility scores and EQ-5D-VAS scores in Europe and the US were numerically lower across all treatment subpopulations for patients with not well-controlled asthma versus patients with well-controlled asthma (EQ-5D utility: Europe, 0.82–0.86 vs. 0.97; US, 0.85–0.86 vs. 0.94–0.96; EQ-5D-VAS: Europe, 67.13–68.58 vs. 82.16–84.94; US, 73.90–74.76 vs. 85.19–87.92) (Fig. 5).
Fig. 5: EQ-5D utility and EQ-5D-VAS scores stratified by asthma control status and treatment group.
a EQ-5D utility and b EQ-5D-VAS scores. Data for Canada, China, and Japan were not collected. A score of 1.0 for EQ-5D utility and of 100.0 for EQ-5D-VAS denote the best health state. ACT Asthma Control Test, EQ-5D EuroQol 5 dimensions, ICS inhaled corticosteroid, LABA long-acting β2-agonist, MART maintenance and reliever therapy, SD standard deviation, US United States, VAS visual analog scale.
Comments (0)