
Remember me
Our study used two regional linkable administrative databases of Lombardy to conduct a retrospective observational study. Lombardy is a northern Italian region with about 10 million inhabitants, accounting for over 15% of the Italian population. One database included information on demographic data, drug prescriptions, and hospital records of all Lombardy’s residents. The second one is a registry of patients with a confirmed diagnosis of SARS-CoV-2 infection, containing information on hospital admissions and deaths due to COVID-19. A unique identification code allowed the linkage of both databases.
Healthcare in Italy is publicly funded for all residents, irrespective of their social class or employment, and every resident is assigned a personal identification number that is kept in the National Civil Registration System. All residents are assisted by general practitioners under the National Health System. To ensure privacy, each identification code was automatically deidentified. The inverse process is allowed only by the Regional Health Authority on request from judicial authorities. According to Italian law, studies using retrospective aggregated data from administrative databases that do not involve direct access by investigators to individual patient data do not require approval, notification from an Ethics Committee/institutional review board, or patient informed consent.
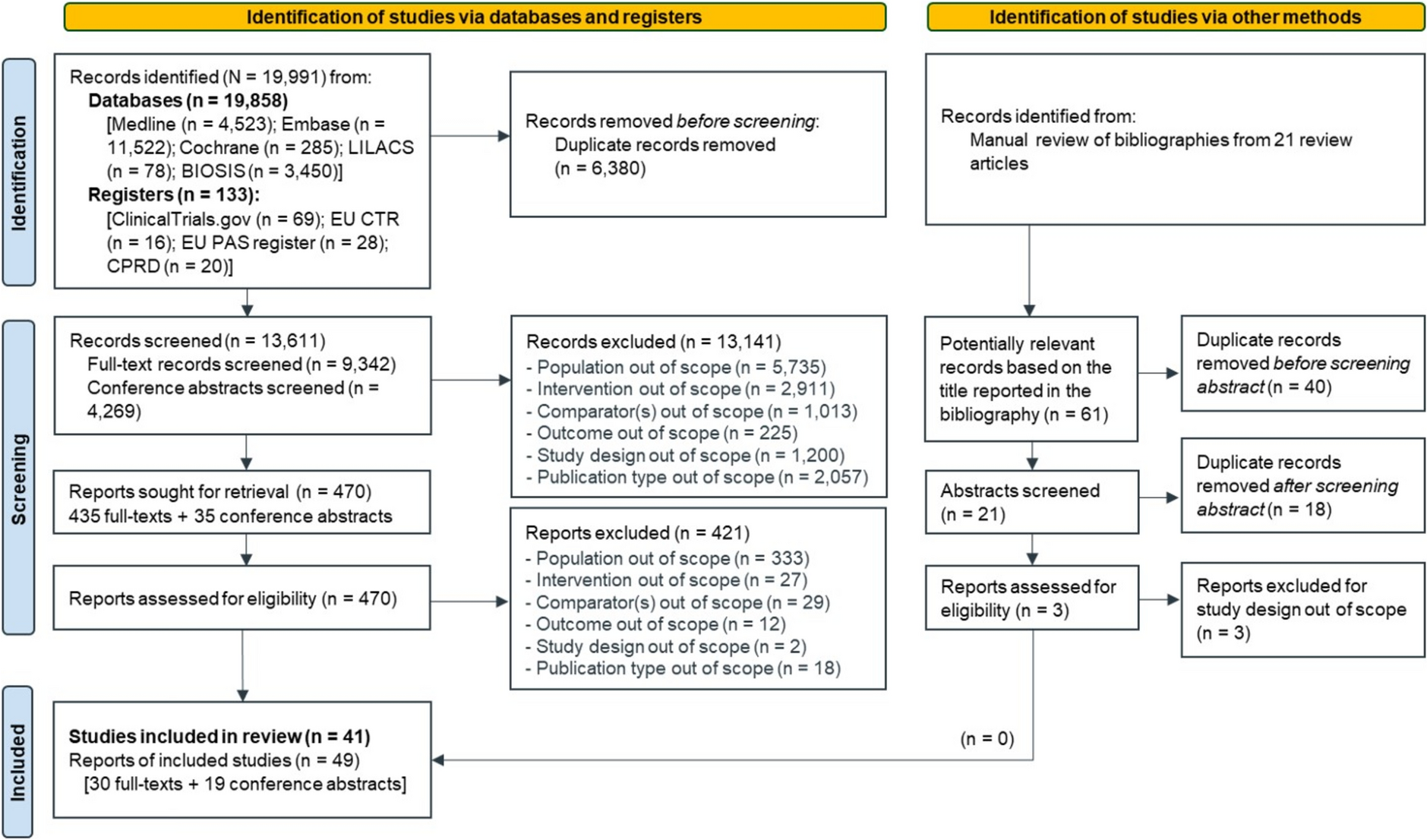
Study PopulationWe selected patients aged 40 years and older hospitalized in Lombardy for COVID-19 from February 1, 2020 to August 31, 2021. The index date was defined as the first date of hospital admission for COVID-19. Individuals who were alive 90 days after the first COVID-19-related hospital admission were included in the following analyses. Since some evidence indicates that viral shedding beyond 80 days is rare, and the virus is cleared in most cases within 30 days from symptom onset [12], we defined rehospitalized patients as those subjects who were hospitalized a second time because of COVID-19 at least 3 months (90 days) after the first admission for COVID-19, likely because of an infection caused by a different SARS-CoV-2 variant (Fig. 1).
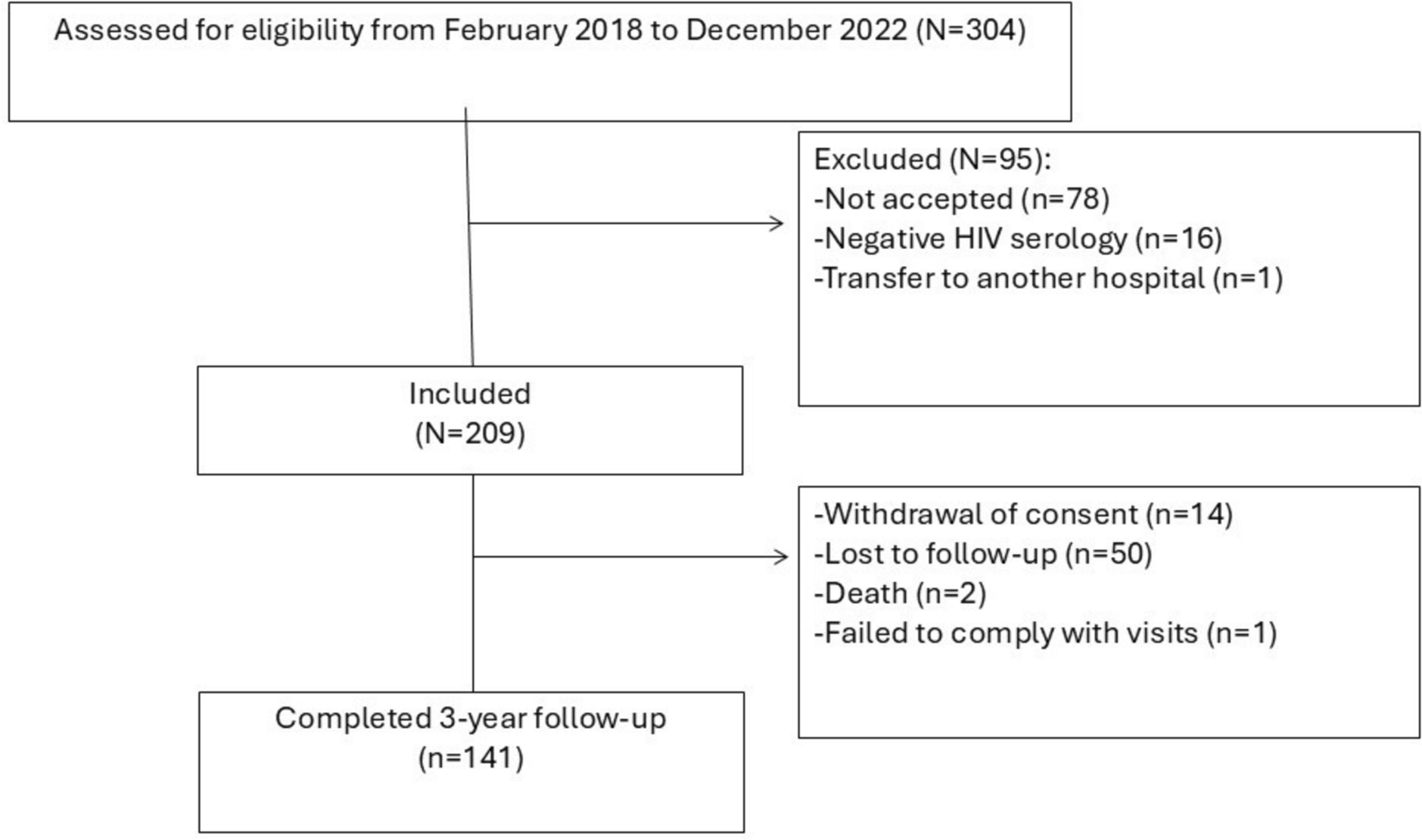
Fig. 1
Study flow chart and timeline. The graph illustrates the number of patients included in the study and in each sub-group (A) and the follow-up timeline for each patient (B)
Intrahospital Mortality, ICU Admission, Comorbidities, and Other CovariatesDemographic data were recorded at the time of inclusion. Access to the ICU and intrahospital mortality (hospitalization outcomes) were collected for the first and subsequent COVID-19 hospital admissions. The history of comorbidities (cerebrovascular disease, heart disease, venous thromboembolism, renal disease, lung, and liver diseases) in the 5 years before the index date was assessed using medical records by annotating both the primary diagnosis as well as up to five coexisting conditions. Diabetes mellitus was evaluated based on at least two prescriptions of antihyperglycemic drugs in the 2 years before the index date. Disease-associated immune suppression was gathered using hospitalization for cancer (in the 5 years before the index date), prescriptions for antiretroviral drugs, and immune suppressive treatments (in the 2 years before the index date) (Supplementary Tables S1 and S2). Finally, a comorbidity count was established with the following categories based on the number of identified comorbidities: 1, 2, 3, ≥ 4.
Exposures to medications of interest (cardiovascular drugs, drugs for respiratory disease, and steroidal anti-inflammatory drugs) were also traced in the 2 years before the index date. Hospitalizations and pharmacy prescriptions were classified according to the International Classification of Diseases, ninth revision, and Anatomic Therapeutic Chemical classification code, respectively (Supplementary Tables S1 and S2).
Study Outcomes and Follow-UpThe outcome of the study was determining the risk factors for rehospitalizations due to COVID-19 in the follow-up period starting at least 90 days after the first COVID-19-related admission. This 3-month window was chosen as likely indicative of a different SARS-CoV-2 infection [12]. The follow-up started 90 days after the index date and proceeded up until the minimum date between the date of death, the date of the rehospitalizations, or the end of the observation period (March 15, 2022, Fig. 1).
Statistical AnalysesThe baseline characteristics of the rehospitalized and non-rehospitalized patient groups were described as follows: continuous variables were reported as median and interquartile range (Q1–Q3) while dichotomous variables as frequencies and percentages. Baseline continuous variables were compared using a t-test, and categorical variables were compared with a χ2 test.
The Fine-Gray subdistribution hazard model was used to estimate the probability of being rehospitalized due to COVID-19 considering all-cause death as a competing risk. In this analysis, patients who died within 90 days after the first hospital admission were not censored. The association between baseline characteristics and outcome occurrence was reported as hazard ratio (HR) with 95% confidence intervals (CIs). The HR was calculated taking death into account as a competing event. Two different models were implemented; in the first model, the HR was adjusted for all covariates collected at baseline (age, biological sex, ICU, comorbidities, and medications), while in the second model, age, biological sex, comorbidity count, and medications were considered.
A p value < 0.05 was used for statistical significance. All analyses were done using SAS version 9.4 (SAS Institute).
Patients Hospitalized and Rehospitalized Because of COVID-19A total of 98,369 individuals were hospitalized for COVID-19 in Lombardy between February 1, 2020 and August 31, 2021. Most patients were male patients (57,813, 58.8%) and belonged to older age groups (median age, 71.8 years, IQR 58.3–81.6). The most frequently observed comorbidities were diabetes (16.3%), immune suppression (14.0%), and heart diseases (12.9%). Overall, 25.7% of patients had a presumed history of at least one comorbidity. A large proportion of patients had prescriptions for at least one of the considered medications during the 24 months before hospital admission, with angiotensin-converting enzyme (ACE) inhibitors being the most common (Supplementary Table S3). Overall, only 348 patients (0.4%) received a vaccination against SARS-CoV-2. A total of 25,776 hospitalized patients (26.2%) died within 3 months after the hospital admission, with 86.2% of them (22,213/25,776) dying during the hospitalization period (corresponding to an intrahospital mortality rate of 22.6%, 22,213/98,369).
Figure 1 shows the study flowchart. Overall, 72,593 subjects were alive after the first hospital admission and were, therefore, included in the analyses. Of these, 71,983 were never rehospitalized because of COVID-19 during the study period while 610 (0.8%) were rehospitalized for COVID-19 at least 90 days after the first hospitalization, suggesting a likely novel SARS-CoV-2 infection. Finally, 97 died during the second hospitalization (corresponding to an intrahospital mortality rate during the second hospitalization of 15.6%). Similarly to intrahospital mortality rates, ICU admissions were also reported more frequently during the first hospitalization compared to the second admission (4.2% vs. 2.5%). Only two patients were rehospitalized for COVID-19 a third time (at least 90 days after the second COVID-19-related admission). Additionally, rehospitalized patients were old (75.7 years, IQR 74.4–83.1), and only 1.8% of them were admitted to the ICU during the first hospitalization. The rate of patients admitted to the ICU during the first hospitalization was similar between the two groups of non-rehospitalized and rehospitalized patients that were alive at 3 months after the first hospitalization (1.7% vs. 1.8%, Table 1).
Table 1 Baseline characteristics of patients hospitalized for COVID-19 and alive at 90 days after admission categorized in non-rehospitalized and rehospitalizedOnly 41% (29,573/71,983) of non-rehospitalized patients were first admitted to the hospital during the first pandemic wave (from February 1 to September 28, 2020) while this was true for 83.3% (508/610) of subjects in the rehospitalized group (p < 0.01).
Risk Factors Associated with COVID-19 RehospitalizationThe comparison between the non-rehospitalized and rehospitalized groups is shown in Table 1. Readmitted patients were older (median age 76 years 67 vs, p < 0.001) and were mostly male patients (61.3%).
The most prevalent comorbidities were heart disease, diabetes mellitus, and disease-associated immune suppression, with a higher comorbidity prevalence in rehospitalized patients (p < 0.001). A significantly higher exposure to medications was also seen in rehospitalized patients (all p < 0.001).
Figures 2 and 3 report the adjusted forest plots for two different models, the first adjusting the HR for all covariates collected at baseline and the second adjusting for age, biological sex, comorbidities count, and medications. A statistically significant association was observed between the risk of being rehospitalized and most of the analyzed variables. The presence of renal failure (HR = 1.8; CI 95% 1.386–2.454), liver disease (HR = 2.1; CI 95% 1.413–3.216), and use of diuretic drugs (HR = 1.6; CI 95% 1.312–1.997) were linked to the highest risk of rehospitalizations for COVID-19. A lower risk was associated with female biological sex and the use of lipid-lowering drugs (Fig. 2).
Fig. 2
Adjusted hazard ratios (HZ) and 95% confidence intervals (CI 95%) of being rehospitalized (model 1) for COVID-19 at least 90 days after the first admission. Abbreviations. ICU intensive care unit, VTE venous thromboembolism, ACE-I angiotensin-converting enzyme inhibitors, ARBs angiotensin II receptor agonist blockers
Fig. 3
Adjusted hazard ratios (HZ) and 95% confidence intervals (CI 95%) of being rehospitalized (model 2) for COVID-19 at least 90 days after the first admission. Abbreviations. ICU intensive care unit, ACE-I angiotensin-converting enzyme inhibitors, ARBs angiotensin II receptor agonist blockers
In the second model, the coexistence of four or more comorbidities was associated with a very high risk of rehospitalizations (HR 5.02, CI 3.21–7.85). A statistically significant increased risk was also observed for patients treated with diuretics, antiplatelet drugs, and drugs for respiratory disease, while a lower risk was seen in female patients and patients who were prescribed lipid-lowering drugs, similarly to what was observed in model 1 (Fig. 3).
Comments (0)