
Remember me
We modeled the outcomes and costs related to the treatment of patients with EC or GEJC who have residual disease after neoadjuvant CRT followed by R0. Adjuvant treatment with nivolumab was compared with the recommended French clinical practice at the date of submission, consisting of patient surveillance.
This SoC was further confirmed by an ad-hoc analysis of a cohort of patients included in the FREGAT (French EsoGastric Tumours) clinic-biological database (ClinicalTrials.gov identifier: NCT02526095) [11]. This prospective national database consists of a French multicenter (N = 35 centers) cohort of esophago-gastric cancers of any tumor stage or therapeutic strategy. Patients diagnosed with a resectable stage II or III EC or GEJC were identified between 2014 and 2019 (N = 1366). Of these, 947 patients underwent surgery. Among them, 382 had received neoadjuvant CRT and were included in the FREGAT cohort for the present analysis. Of these, 362 (95%) did not receive active treatment. Similarly, among the patients who matched CheckMate 577 inclusion criteria (non-pathological complete response, R0 resection, n = 246), 232 (94%) received no treatment after tumor resection [12].
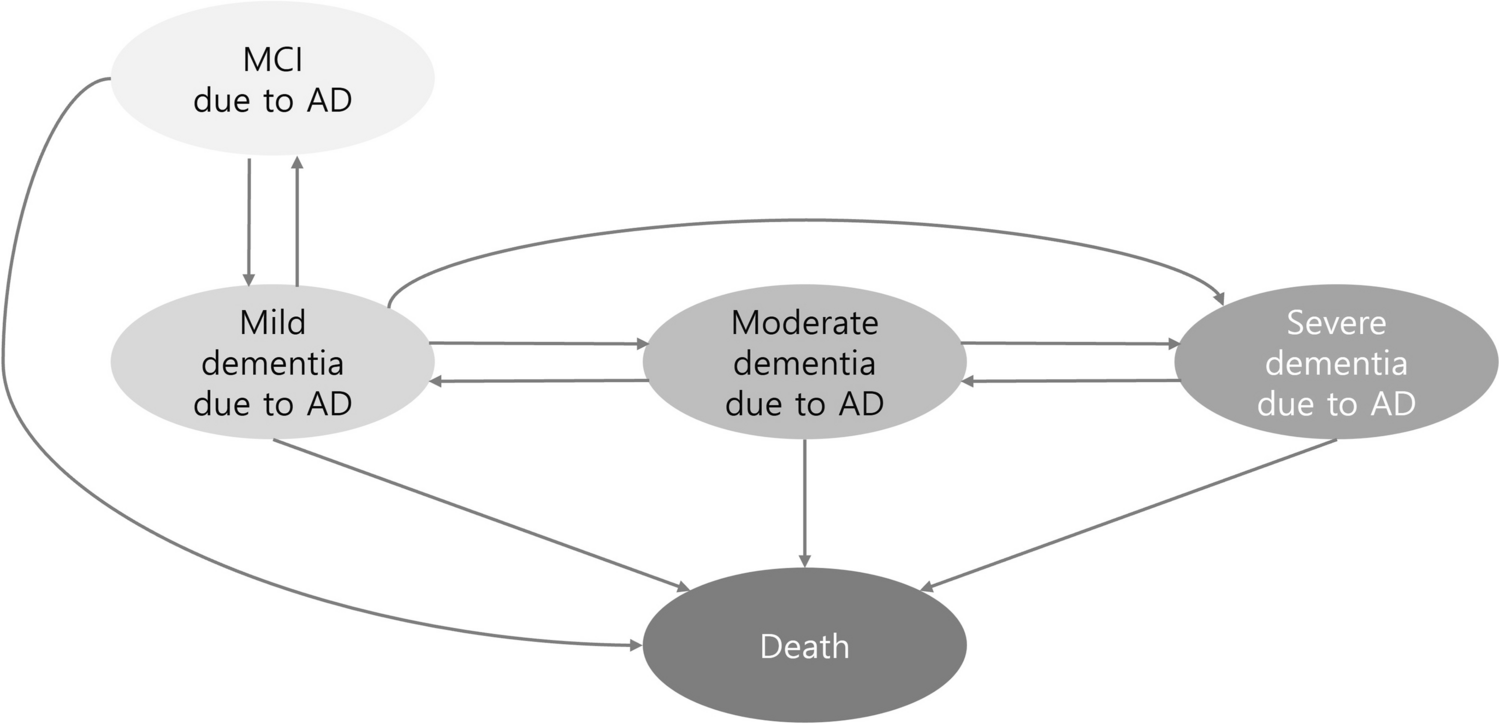
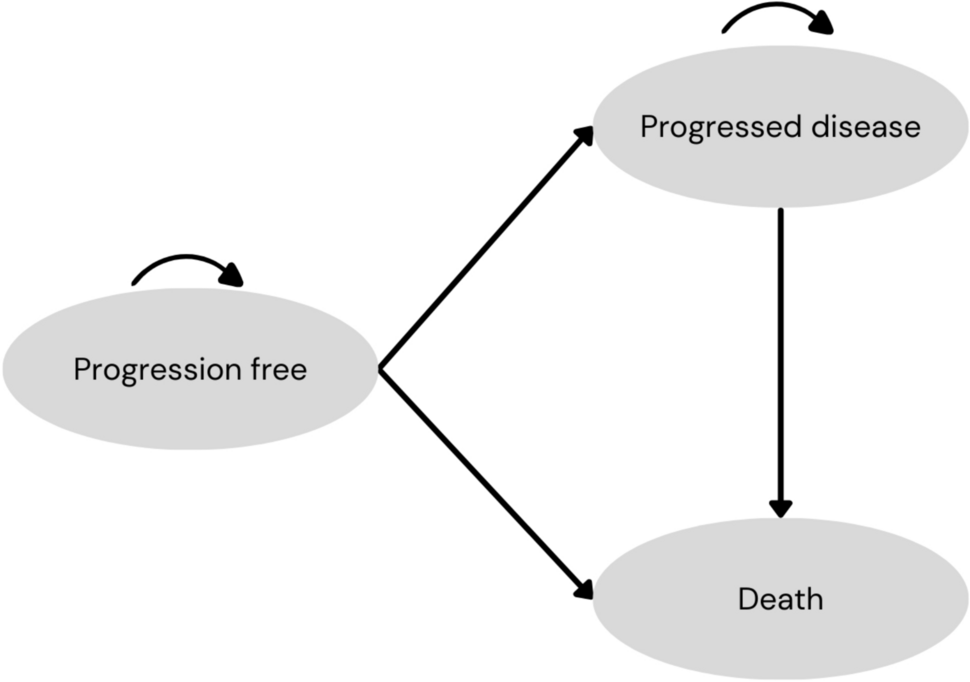
2.2 Model StructureA homogenous Semi-Markov model with a 4-week cycle (consistent with nivolumab frequency of administration) was applied containing a time-dependent part to model the incidence of recurrence as a function of the time, with four simplified health states: disease-free (DF), locoregional recurrence (LR), distant recurrence (DR), and death (Fig 1). The four-health-state structure allowed us to model the distribution of the types of recurrences (locoregional, distant) based on CheckMate 577 results and to account for their specific survival, costs and outcomes. A Markov-type model was preferred over the partitioned survival model typically used in oncology because, at this stage of the disease, patient follow-up must be sufficiently long to observe a significant number of events, such as death since randomization. At the latest database lock of CheckMate 577, OS data since randomization were not sufficiently mature to be extrapolated. A partitioned survival model would have therefore required making strong assumptions of correlation between DFS and OS. Therefore, considering the immaturity of OS data from CheckMate 577, the predominance of the use of Markov models for evaluating the efficacy of adjuvant therapies, and the different distribution of recurrence types between the trial and external data sources (Netherland Cancer Registry [NCR] and FREGAT study) allowing determination of transition probabilities for the model, a simplified four-health-state Markov model was used in the reference analysis.
Fig. 1
Simplified, four-health-state homogenous semi-Markov model structure
A unique transition into post-recurrence states characterizes the occurrence of a first LR or DR state for patients. These locoregional and distant recurrences are distributed according to CheckMate 577. Furthermore, no transition between LR and DR was considered as there was no data available in the literature or in CheckMate 577 to inform this transition.
Lacking mature post-recurrence survival data from the trial implied the use of an external source to inform the transition between post-recurrence states and death [13]. These transition probabilities are specific to the type of recurrence and independent of treatment arm. This hypothesis suggests that nivolumab only has an impact on the risk of recurrence as post-recurrence survival is equal between arms.
Patients entered the model in the DF health-state. Time-dependent DF-to-recurrence transition was informed by a parametric extrapolation of the treatment-specific time-to-recurrence (TTR, derived from CheckMate 577 mortality-censored DFS), applying distribution between locoregional and distant recurrence observed in the trial.
Patients could also die without recurrence based on the age- and sex-matched general population mortality. An ad-hoc analysis compared the mortality of patients without recurrence from CheckMate 577 to that of the general French population. The results confirmed excess of mortality among patients in the indication who had not experienced recurrence and estimated it with an HR of 3.46 (95% CI 2.53–4.74]. The calculation of this HR is based on the number of patients at risk of death without recurrence over the 4-year follow-up of CheckMate 577 and mortality data in the general French population adjusted by age and sex ratio. Using this data, the Kaplan-Meier estimator was determined to generate individual mortality data according to the Guyot algorithm. These individual mortality data were compared with pre-recurrence mortality outcomes in the CheckMate 577 trial using Cox methods to determine an HR and a 95% confidence interval. It was assumed that treatment did not affect this transition.
A 15-year time horizon, chosen due to the median age of inclusion of patients at resection (60.5 years), the natural history of the disease at this stage and to limit uncertainty beyond, was simulated for population-matched patients included in the trial. Costs and outcomes were discounted by 2.5% per year.
2.3 Survival in Disease-Free Health-StateSchoenfeld residuals, cumulative hazard plot, and log-log survival plot confirmed that hazards of recurrence between nivolumab and surveillance were not proportional. Thus, unrestricted parametric distributions were fitted independently to CheckMate 577 TTR data and selected based on Akaike and Bayesian Information Criteria (AIC and BIC), visual inspection, and external validity using literature.
In both arms, Generalized Gamma (reference analysis) and Gompertz (‘cure’ scenario) distributions offered the best fit, the former being more pessimistic, whereas Gompertz distributions plateaued from 6 years, consistent with the notion that patients who have not recurred after 5 years in the adjuvant context may have limited to no chance of recurrence. Nevertheless, in the absence of external validation of this assumption, the more conservative Generalized Gamma distribution was favored in the reference analysis (Fig. 2).
Fig. 2
Gen Gamma (reference analysis) and Gompertz (‘pseudo-cure’ scenario) distributions for time-to-recurrence deriving proportion of patients still alive without any recurrence over time—nivolumab and surveillance arms in resected esophagal cancer/gastroesophagal junction cancer
Furthermore, given the uncertainty surrounding nivolumab’s efficacy in the long term, the risk of recurrence in the nivolumab arm was progressively increased to reach the same level as in the surveillance arm at the end of the simulation, starting at 5 years.
2.4 Survival in Locoregional Recurrence (LR) and Distant Recurrence (DR) Health StatesConstant probabilities of death in the LR and DR health states were estimated based on an unpublished ad-hoc analysis of 359 adult EC and GEJC patients from the Netherlands Cancer Registry (NCR) who were diagnosed in 2015 or 2016 and met CheckMate 577 inclusion criteria. A similar analysis from the NCR has since been published [13]. Constant hazards were fitted to recurrence-specific mortality data of 332 and 27 patients with distant and locoregional recurrence, respectively. NCR was favored over FREGAT to inform the recurrence-specific mortality due to the limited number of patients (N = 13) with locoregional recurrences identified in the ad-hoc analysis from the FREGAT database. Other potentially appropriate sources were discarded for the same reason [14, 15].
2.5 Utility and CostsSurvival in each health state was associated with utilities derived from the EQ-5D-3L results of CheckMate 577 valued according to the preferences of the French general population [16] (Table 1) to characterize the impact of disease progression on patients' health-related quality of life. In the absence of significant utility differences between nivolumab and surveillance, the health-state-specific utilities from the intention-to-treat population were preferred in the reference analysis.
Table 1 French utility values derived from CheckMate 577 EQ-5D-3L results by health state and populationHealth-state occupancy, recurrences, and deaths were associated with medical resource uses estimated based on existing guidelines.
As recommended within HAS guidelines for cost-effectiveness analysis in France, a collective perspective excluding indirect costs valued based on production costs and an annual discount rate of 2.5% for costs and outcomes was adopted [17].
Treatment acquisition and administration, disease monitoring, management of treatment-related adverse events (TRAE) of grade 1–4 with an incidence of at least 1% for the nivolumab arm, cost of subsequent treatments, transportation, and end-of-life care were considered.
Treatment acquisition costs were calculated by considering French public prices (all taxes included) and the administration schedule. Hospital stays associated with administration costs, management of TRAE and end-of-life care were calculated based on French hospital costs. All costs were updated to 2021 euros according to the French consumer price index [18]. No indirect or opportunity costs were considered in the model.
Subsequent treatment distribution for patients with recurrence was modeled based on CheckMate 577, distinguishing treatment arms and type of recurrence. A comparable distribution of patients received subsequent treatment at progression in CheckMate 577. Most patients were treated with chemotherapy and three regimens could be identified: 5FU+cisplatin, capecitabin+oxaliplatin (CAPOX), and 5FU+oxaliplatin (FOLFOX) (Table 2).
Table 2 Distribution of subsequent treatment regimens after recurrence from CheckMate 577 and FREGAT (French EsoGastric Tumours study)The rate of patients treated by chemotherapy or radiotherapy in CheckMate 577 is consistent with French practice observed in the FREGAT cohort. Although this study does not detail certain chemotherapy regimens based on the type of recurrence due to lack of power, the proportions of patients treated with radiotherapy, chemotherapy and FOLFOX regimens are similar to those observed within CheckMate 577. The use of surgery after recurrence was less compared with that in CheckMate 577.
2.6 Sensitivity AnalysisThe list of parameters and their ranges are presented in the electronic supplementary material (ESM, Table S.1). The robustness of results was evaluated with deterministic and probabilistic sensitivity analyses (DSA and PSA) as well as through different scenario analyses with varying time horizons, absence of treatment effect waning after 5 years, modeling a 5-year ‘cure’, or using a Gompertz function to model TTR that reflects a ‘pseudo-cure’ assumption after 6 years. This cure assumption is justified by the decreased risk of recurrence observed in both CheckMate 577 arms as well as the results of several real-world studies showing that OS and DFS of patients who did not experience recurrence after 4 or 5 years plateaued at around 30–40% [14, 15, 19, 20].
Furthermore, given the uncertainties related to the probabilities of transitions between LR and DR as well as the risks of recurrence-specific mortality probability, several scenarios using a homogenous semi-Markov structure with three health states, without distinction between types of recurrence, based on post-recurrence survival and subsequent treatment from NCR and FREGAT databases were realized. As the FREGAT study does not detail the rate of subsequent treatments according to treatment arms, the proportion of patients receiving subsequent treatments among those who have recurred is based on data from CheckMate 577. The same applies to the distribution of chemotherapy regimens, which was not available in the FREGAT study.
Comments (0)