Tracheal resection or crico-tracheal resection anastomosis has been established as the definitive surgical management for high grade post-intubation subglottic stenosis. The procedure had been continuously updated to achieve a relaxed tension free anastomotic closure especially in cases with challenging long stenotic segment. A major limitation in cases of tracheal resection is the length of the stenotic segment and subsequently, the tension created on the tracheal ends of the anastomosis. With resection lengths of less than 2–3 cm, no additional manoeuvres are usually needed to bring the two anastomotic ends together, but these situations are not often the case. In 1948, Rob and Belsey proposed a 2 cm length limit to be the extent for primary tracheal resection and reconstruction [17, 18].
The understanding of the surgical technique and the anatomical structures involved can result in a tension free and well-perfused anastomosis [19]. It is reported by Broussard and Mathisen that neck flexion and Para tracheal dissection can allow to resect up to 4 cm of the trachea without anastomotic complication [20]. Yet, patients with longer tracheal lesions handled by either limited surgical options or anastomotic complications following aggressive surgery. So, additional release techniques were employed to extend the tracheal resection limit up to 6 cm [1, 20, 21]. Rosen et al. [22] found that by using an appropriate laryngeal drop technique, about 6.68 cm, 13.3 tracheal rings or 65.5% of the total tracheal length can be removed without creating tension on the anastomosis.
A different tracheal release procedures were reported as suprahyoid, infrahyoid and paracardial release manoeuvres [20]. These release manoeuvres can affect longitudinal pharyngeal muscles that assist in pharyngeal expansion and constriction during swallowing. Other possibly affected muscles are the suprahyoid muscles including the digastric, geniohyoid, stylohyoid, and mylohyoid, as well as the infrahyoid muscles such as the omohyoid, sternohyoid and thyrohyoid, which are responsible for elevation and depression of the hyoid bone, respectively, during swallowing.
Affection of these muscles had been associated with dysphagia in the early postoperative period following tracheal resection [23, 24]. While recent studies have identified various surgical factors that contribute to dysphagia following airway resection surgery, few reports concerned with discussing the difference in swallowing outcomes according to the method of laryngeal release used [25].
Dedo and Fishman [26] described the infrahyoid laryngeal release in 1969. The technique involved dividing the thyrohyoid muscles, thyrohyoid membrane and the superior horns of the thyroid cartilage. Grillo et al. reported that 2.5 cm of proximal tracheal mobilization can be achieved with infrahyoid laryngeal release in a series of 49 cases. This was associated with swallowing problems in about 1.2% of cases [1]. Maassen [27] also reported some transient swallowing problems after infrahyoid laryngeal release.
Suprahyoid release was discussed in 1974 by Montgomery et al., [28] in which the mylohyoid and geniohyoid muscles were detached from body of the hyoid bone, which was then separated from the greater and lesser cornu. This procedure allows for pulling down the proximal trachea by about 2–3 cm [29]. Transient swallowing dysfunction occurred in 17 (32.2%) patients reported by Mohsen et al., exclusively in patients who underwent laryngeal release. Notably, this dysfunction was temporary and relieved in the early postoperative period [30].
In the current study, a comparison between two techniques of infrahyoid laryngeal drop was conducted. These two techniques are considered mini or full drop after the preservation or fracture of the superior thyroid horn bilaterally. The final swallowing outcomes were significantly better in the mini release group with greater severity of swallowing difficulties in the full group. In a previous study, the length of the resected trachea and hence the need to do more laryngeal release did not cause dysphagia or affect diet after the surgery [11].
In the current study, a correlation between older patients’ age and worse swallowing outcomes was found in the group having a full laryngeal drop. Christopher et al., concluded similar results in their study in which there was an association between patient age and swallowing scores, suggesting that the age could increase the severity of dysphagia after tracheal resection and delay the return to normal preoperative diets [11]. This can be explained by their lower baseline functional status with expected greater postoperative functional deficit after disruption of the normal swallowing mechanism during surgery. Given the existing literature, it has been found that disruption of soft tissues during laryngeal drop in tracheal resection in patients of increased age contributes to greater postoperative affection of swallowing and prolonged dysphagia. So, patients of advanced age should be counselled to expect swallowing difficulties especially if a full laryngeal drop was implemented [31,32,33].
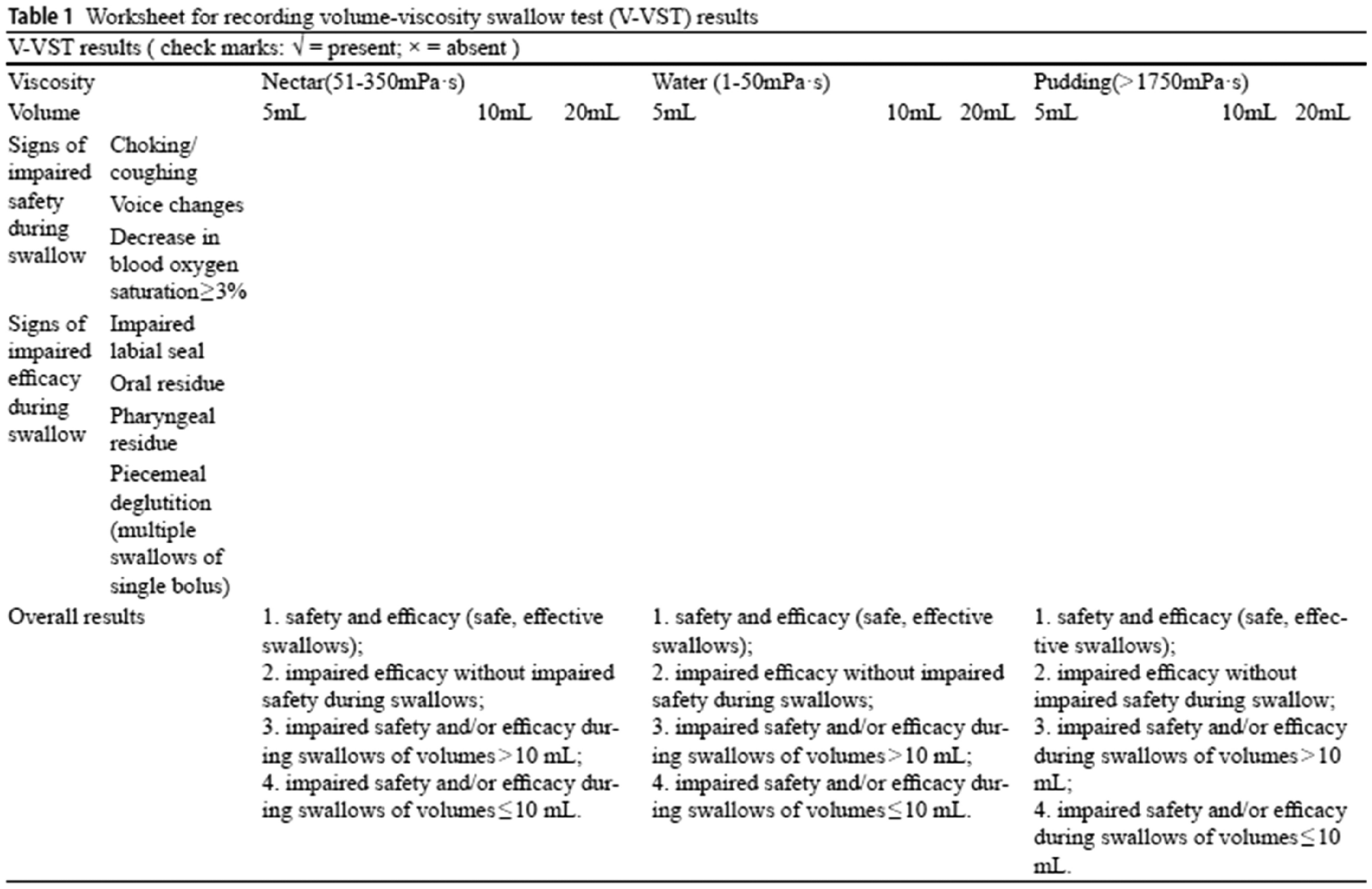
The current study has some limitations. Its retrospective nature made data collection limited to the previously available recorded variables. Also, swallowing outcomes were evaluated in the immediate post-operative period (one month). The fact that makes the long-term functional outcomes still unclear. Therefore, future studies should be performed with structured observation and a long-term follow-up period. Additionally, our results revealed that GUSS test has a high sensitivity in evaluation of swallowing outcomes. This is of a notable importance as GUSS test is easier to implement than FEES. However, this result, being based on a retrospective study, needs to be furtherly investigated using prospective comparative studies to have a more accurate validation.





Comments (0)