
Remember me



A cohort of 50 patients with mGB with a total of 181 tumor lesions (mean number of tumor lesions per patient, 3.6 ± 1.5; range, 2–7) and a cohort of 50 patients with mCNSL with a total of 187 tumor lesions (mean number of tumor lesions per patient, 3.8 ± 2.4; range, 2–10) were analyzed. The mean age of the mGB subgroup was 65 ± 13 (range, 36–91) years; 68% (34/50) were male, and 32% (16/50) were female. In the subgroup with mCNSL, the mean age was 63 ± 25 (range, 35–81) years; 56% (28/50) were male, and 44% (22/50) were female. PNSCL was diagnosed in 38 patients (76%), and SCNSL was diagnosed in 12 patients (24%). Histologically, malignant diffuse B-cell non-Hodgkin lymphoma was diagnosed in all 50 patients. The baseline characteristics are summarized in Table 1. Typical examples of mCNSL and mGB are shown in Fig. 2 and Fig. 3.
Table 1 Imaging characteristicsFig. 2
Example of a patient with CNS lymphoma with multiple lesions (mCNSL). Top: contrast-enhanced T1 sequence, showing periventricular tumor growth affecting the basal ganglia, brain stem, and the left hippocampus. Middle: fluid inversion recovery (FLAIR) sequence demonstrating the signal of tumor lesions and perilesional edema. Bottom: diffusion weighted imaging (DWI) with the apparent diffusion coefficient (ADC) indicating a diffusion restriction of the lesions
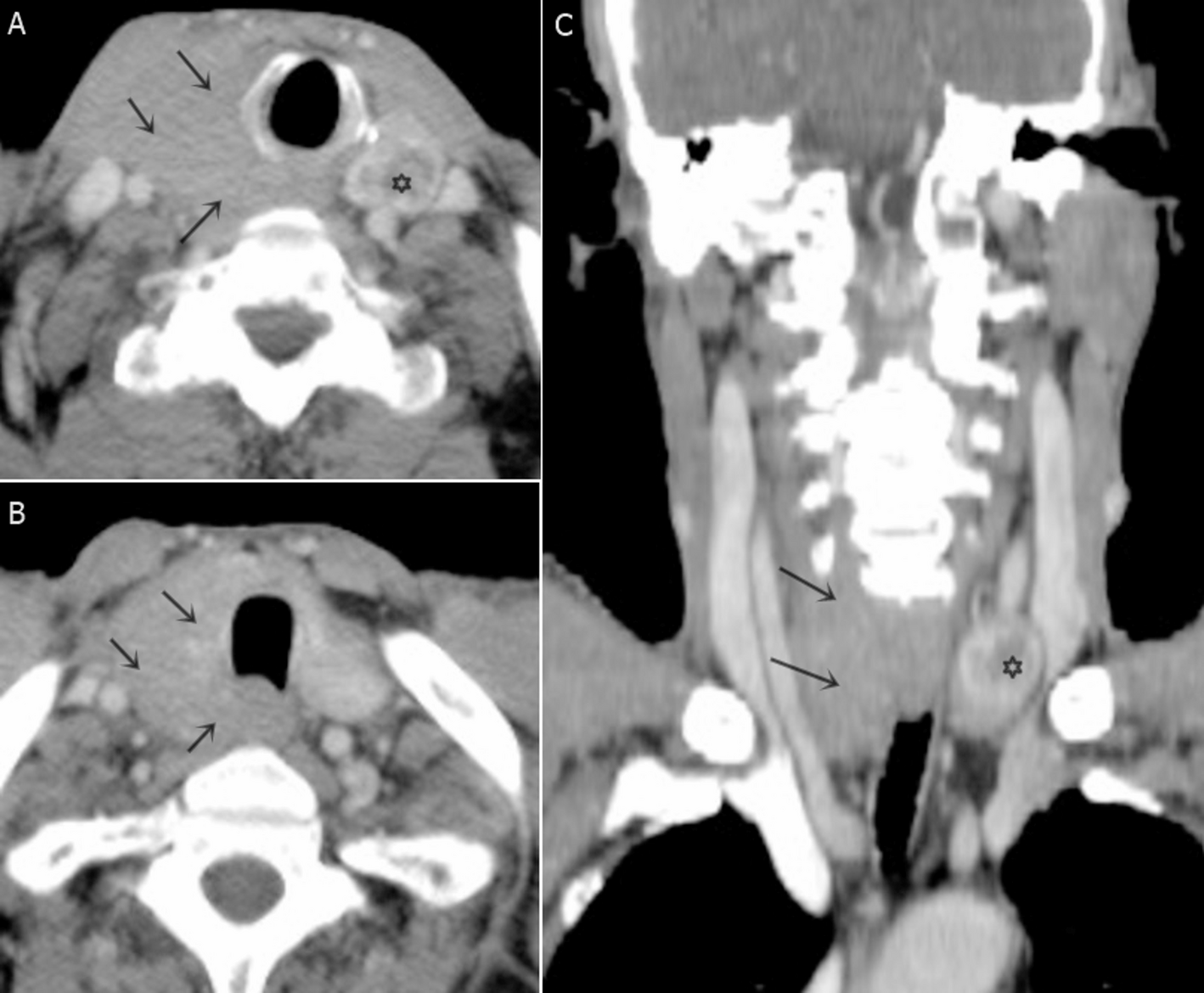
Fig. 3
Example of a patient with mGB. A Contrast-enhanced T1 sequence showing three separate tumor lesions. B Fluid inversion recovery (FLAIR) sequence demonstrating the tumor infiltration zone within the perilesional region. C Diffusion weighted imaging (DWI) with the apparent diffusion coefficient (ADC) showing higher ADC values within the tumor lesions but lower ADC values within the perilesional regions
3.2 Radiological characteristics of GB with multiple tumor lesionsContrast enhancement was found in 77 ± 28% of mGB lesions per patient (range, 0–100%; median, 100%). In 94% (47/50) of mGB cases, the tumor lesions were found to have a supratentorial location, whereas only 6% (3/50) had an infratentorial location. The mean measured diameter on contrast-enhanced T1-weighted sequences of mGB tumor lesions was 24.8 ± 16.0 mm (range, 2–83 mm).
The 181 mGB tumor lesions were morphologically classified as follows: 25 (14%) solid; 25 (14%) mixed, with cystic and solid parts; 65 (36%) cystic; 66 (36%) diffuse cortical infiltration; 0 (0%) stripe- or tree-shaped; and 0 (0%) extra-axial. The mean measured diameter (T2-/FLAIR-hyperintensity) of perilesional edema in patients with mGB was 6.6 ± 8.4 mm (range, 0–40 mm; median, 3 mm). Sixty-three per cent (114 of 181) of mGB lesions were FLAIR-connected to at least one other lesion. The overall mean measured distance between individual tumor lesions in all patients with mGB was 14.0 ± 14.4 mm (range, 1–73 mm; median, 5 mm).
MRI perfusion was available in 74% (37/50) of patients with mGB bearing 134 tumor lesions. An increased rCBV was detected in 85 of 134 (63%) mGB tumor lesions. An SWI sequence was performed in 28% (14/50) of patients with mGB bearing 51 tumor lesions. Hemorrhage was found within 14% (7/51) of assessed tumor lesions, whereas 8% (4/51) of evaluated lesions showed increased vascularization on the SWI sequence. An overview of imaging characteristics in the patient subgroup with mGB is given in Table 1.
3.2.1 Subgroup analysis—multicentric versus multifocal GBIn 24% (12/50) of patients with mGB, tumor lesions were found without visible T2-/FLAIR-weighted connections between lesions (“multicentric”), and 76% (38/50) had at least one visible connection between tumor lesions (“multifocal”). To clarify whether there are further morphological differences, we performed this subgroup analysis.
In patients with “multifocal” mGB, the mean distance between the lesions was 9.9 ± 10.4 mm (range, 0–44 mm; median, 2 mm), a value significantly shorter than that in patients with “multicentric” mGB 26.5 ± 17.0 mm (range, 0–73 mm; median, 22 mm; t-test p < 0.01). No significant differences among these subgroups were detected in tumor size (“multifocal” mGB, 25.4 ± 16.0 mm; “multicentric” mGB, 22.6 ± 16.2 mm; p = 0.14). Perilesional edema was slightly (but not significantly; t-test, p = 0.42) more pronounced in “multifocal” mGB tumor lesions (5.9 ± 8.8 mm, range, 0–40 mm; median, 4 mm) than “multicentric” mGB tumor lesions (5.8 ± 6.6 mm, range, 0–19 mm; median, 3 mm). The tumor-edema ratio (lesions without edema were excluded) was higher in the “multicentric” mGB subgroup (5.3 ± 4.9; median, 3.9) than in the “multifocal” mGB subgroup (4.1 ± 3.7; median, 2.6), but the difference was not statistically significant (p = 0.17).
3.3 Radiological characteristics of CNSL with multiple tumor lesionsContrast enhancement was found in 88 ± 33% of mCNSL tumor lesions per patient (range, 0–100%; median, 100%). The mean measured diameter of mCNSL lesions on contrast-enhanced T1 sequences was 18.8 ± 14.3 mm (range, 1–64 mm; median, 16 mm). A visible connection between at least two tumor lesions on FLAIR sequences was found in 49% (92/187) of all lesions. In 36% (18/50) of patients, all tumor lesions were connected on the FLAIR sequence, in 28% (14/50) of patients, the tumor lesions were partly connected, and in another 36% (18/50) of patients, the tumor lesions had no visible connection. The mean measured distance between the mCNSL tumor lesions was 22.8 ± 18.7 mm (range, 1–83 mm; median, 20 mm). The mean measured diameter of perilesional edema was 6.6 ± 8.3 mm (range, 0–44 mm; median, 3 mm). The tumor-edema ratio was 3.9 ± 3.7. The mCNSL tumor lesions were morphologically classified as follows: 74% (139/187) were solid; 2% (3/187) were mixed, with cystic and solid parts; 6% (11/187) were cystic; 2% (3/187) exhibited a diffuse cortical infiltration; 15% (28/187) were stripe- or tree-shaped; and 3% (6/187) were nodular and adjacent to the dura. MRI perfusion was available in 34% (17/50) of patients with mCNSL bearing 73 tumor lesions; an increased rCBV was found in 55% (40/73) of tumor manifestations and in 71% (12/17) of patients with mCNSL. The typical time-signal intensity curve with T1-leakage and high percentage of signal recovery (PSR) was detected in 32% (23/73) of mCNSL tumor lesions (53%; 9/17 patients with mCNSL). An SWI sequence was performed in 20% (10/50) of patients with mCNSL bearing 33 tumor lesions. Hemorrhage within the tumor lesions was detected in 36% (12/33) of tumor lesions and 20% (2/10) of patients with mCNSL with SWI sequence available. Increased vascularization was found in 52% (17/33) of tumor lesions and in 60% (6/10) of patients with mCNSL with SWI sequence available at admission. The imaging characteristics in the patient subgroup with mCNSL are shown in Table 1.
3.3.1 Subgroup analysis—primary versus secondary LymphomaTo clarify whether primary and secondary CNS lymphomas differ morphologically, we performed this subgroup analysis. Multi-parameter analysis (n = 20 parameters) indicated significant differences (mPCNSL vs. mSCNSL, significance level 5%) in the number of FLAIR connections per lesion (0.43 ± 0.50 vs. 0.71 ± 0.46, p = 0.0028), distance between lesions (26 ± 19 mm vs. 13 ± 13 mm, p < 0.0036) and tumor-edema ratio (3.5 ± 3.2 vs. 5.1 ± 4.8, p = 0.047). After correction (Bonferroni, significance level set to p = 0.0025), none of these parameters remained significant.
3.4 Differentiation between mGB and mCNSL on initial MRIThe typical time-signal intensity curve with T1-leakage and high PSR was observed only in mCNSL lesions (53% of patients and 33% of tumor lesions), but in none of the mGB tumor lesions (binomial test; p < 0.00000001). Hemorrhage (36% vs. 14%, binomial test; p = 0.00036) and increased vascularization within the tumor lesions (52% vs. 8%, binomial test; p < 0.00000001) were detected significantly more often in mCNSL than mGB tumor lesions. After correction for multiple comparisons (Bonferroni method), the significance level was set to p = 0.0025. Whereas mGB lesions were more often marginal contrast enhancing with central necrosis ("cystic" or "cystic and solid" shaped) or presented similarly to low-grade tumor components (“cortical infiltration”), most mCNSL tumor lesions were solid, but 15% showed a pathognomonic “stripe”- or “tree”-like enhancement. The most observed locations of tumor lesions in both entities were similar. Although both entities were associated with a location involving the corpus callosum, mCNSL showed a relative preference for the crus cerebri, cerebellar peduncles, and basal ganglia.
Although the mean measured distance between the foci of mCNSL significantly differed from the mean measured distances in “multifocal” GB (t-test, p < 0.001), this was not the case in “multicentric” mGB (t-test, p > 0.1). The mean measured diameter of mCNSL tumor lesions was significantly smaller than that in mGB tumor lesions (t-test, p < 0.001). The AUC of mean lesion size for differentiation of mGB and mCNSL was 0.62, with an optimized threshold of < 20 mm for detecting mCNSL (Youden's J; sensitivity, 64%; specificity, 56%). No significant differences between mGB and mCNSL were found regarding edema size and the tumor-edema ratio.
The ADC tumor ratios were significantly smaller in mCNSL than in mGB (t-test, p < 0.001). The AUC of ADC tumor ratio for differentiation between mGB and mCNSL was 0.63, and the optimized threshold was < 0.87 for detecting mCNSL (Youden's J; sensitivity, 59%; specificity, 64%). A significantly higher ADC ratio of perilesional edema adjacent to the tumor (5 mm) was detected in mCNSL than mGB (t-test, p < 0.001). The AUC of the ADC ratio for differentiation of mGB from mCNSL was 0.68, and the optimized threshold was > 1.88 for detecting mCNSL (Youden's J; sensitivity, 62%; specificity, 67%). The more distant ADC ratios (≥ 10 mm) did not significantly differ.
The diagnostic algorithm, as shown in Fig. 4, was built following the rationales: Always consider MR perfusion first. This is followed by properties with a specificity of 100%. Significantly different properties are then arranged in descending order according to Youden’s J.
Fig. 4
Radiological discrimination flowchart summarizing the distinctive radiological parameters and their discrimination power between tumor entities (mGB glioblastoma with multiple foci at presentation, mCNSL central nervous system lymphoma with multiple lesions at presentation)
Table 2 shows the most significant features, evaluated in the decision tree.
Table 2 Significant parameters for the differentiation of multiple CNS lymphoma from mGb3.4.1 Subgroup analysisAlthough the FLAIR ratios of edemas did not significantly differ between mGB and mCNSL, an additional analysis of variance post-hoc test (Tukey’s test) revealed significantly lower FLAIR ratios of perilesional edema in mGB than mPCNSL, but not mSCNSL. The FLAIR values and FLAIR ratios of tumor regions, as well as perilesional edemas, are illustrated in Table 3. The additional subgroup analyses of variance for “multicentric” mGB, “multifocal” mGB, mSCNSL, and mPCNSL are shown in Table 4.
Table 3 Subgroup analysis with emphasis on ADC and FLAIR ratios (mean ± standard deviation)Table 4 Results (p-values) of Tukey’s test (Tukey multiple comparisons of means; 95% family-wise confidence level) of four groups (multifocal mGBM, multicentric mGBM, PNCSL and SCNSL) for T2-FLAIR and ADC ratios
Comments (0)