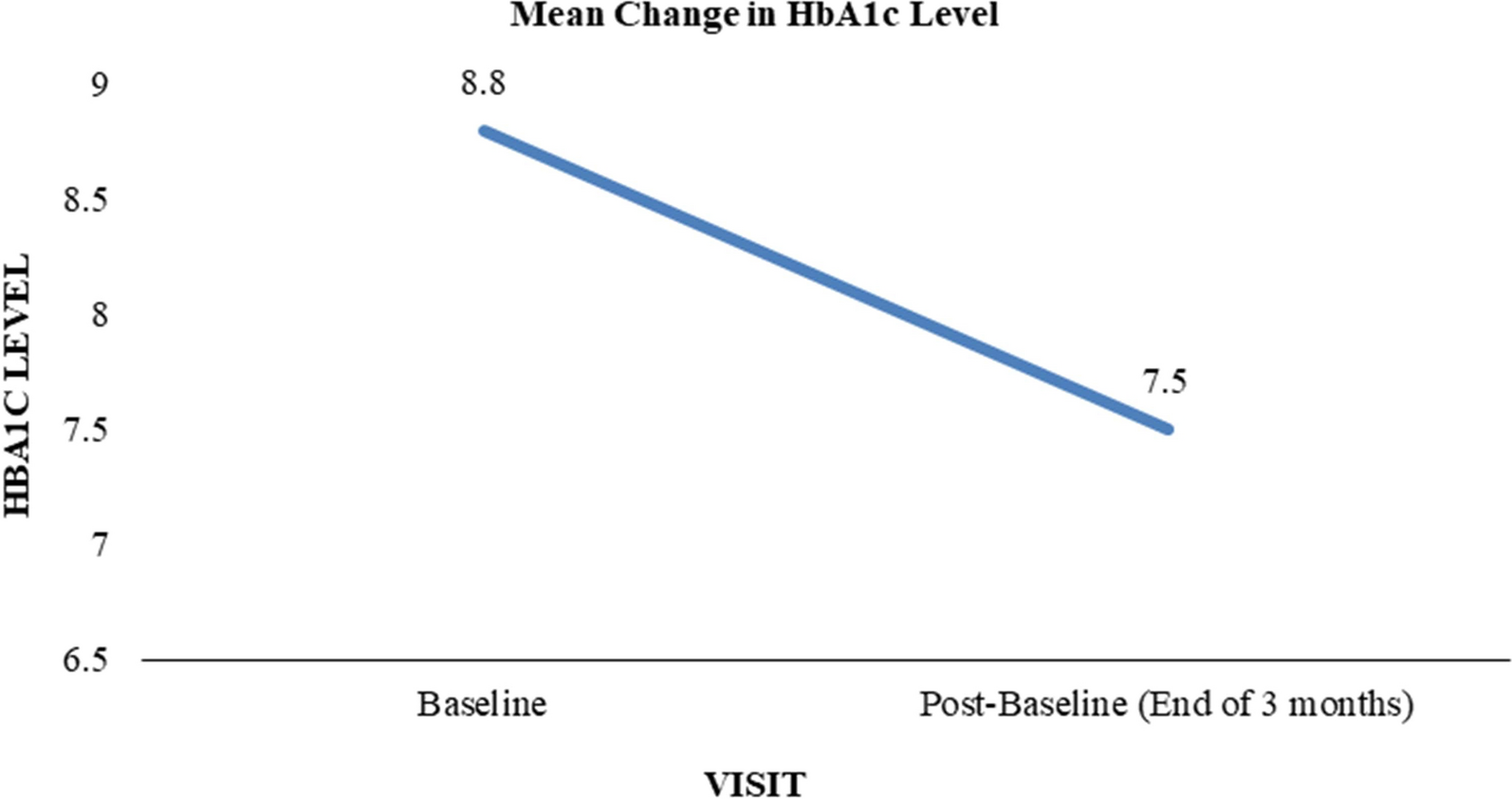
The last decade has a seen a rapid advancement in the development of diabetes technology including CGM. Whilst flash glucose monitoring is widely available for people with T1DM, national recommendations for use in T2DM are more limited [8]. In this real-world retrospective observational study, commencement of the FreeStyle Libre/ Libre 2 Flash Glucose Monitoring System was associated with a clinically significant improvement in HbA1c of 11 ± 14 mmol/mol (1.0% ± 1.3%) at 3–6 months in people living with T2DM treated with multiple daily injections of insulin. This observed improvement supports previous retrospective observational studies in such patients performed in Austria, France, and Germany that demonstrated HbA1c lowered by 8.9–10.1 mmol/mol (0.8–0.9%) at 3 to 6 months [9]. Additionally, a prospective observational study in Italy demonstrated an adjusted difference of − 3 mmol/mol (− 0.3%) compared to matched controls at 3–6 months [10]. Findings from these observational studies are furthered by a randomised controlled trial (RCT) conducted in Israel, which demonstrated an HbA1c reduction of 9 mmol/mol (0.82%) vs. 3.6 mmol/mol (0.33%) in the control group at 10 weeks [11]. On the other hand, a previous European RCT was only able to demonstrate an HbA1c reduction in a subgroup of those aged < 65 years [6]. Potential reasons for the discordance in HbA1c reduction between the previous and more recent RCT could be due to the increased availability of flash glucose monitoring with time [12]. This may have brought about an increased familiarity and understanding of ambulatory glucose profiles (AGPs) amongst patients and clinicians allowing for better management decisions [13]. Differences in results observed between RCTs and observational studies may be due to the real-world setting of observational studies which are less restrictive in terms of their inclusion criteria compared to RCTs [14].
Similar to a previous observational study conducted in Europe, a decrease in HbA1c was observed regardless of age, sex, baseline HbA1c, duration of insulin use or BMI [9]. Whilst the previously discussed RCT only demonstrated an HbA1c reduction in those aged < 65, further studies have demonstrated a reduction regardless of age [9, 11, 15, 16]. It is also noteworthy that a decrease in HbA1c was still observed in those with BMI > 30 given the increasing prevalence of obesity and the additional challenges this presents when managing T2DM [17]. The observed lower HbA1c is likely due to flash glucose monitoring allowing patients to evaluate previously unseen trends in glucose levels. These data may have influenced patients to have better behavioural and lifestyle changes such as increased physical activity and improved food choices [18]. In patients treated with multiple daily injections of insulin, there is a greater risk of recurrent hypoglycaemia, which generally requires de-escalation of insulin therapy and therefore suboptimal glycaemic targets [19]. Whilst not assessed in this study, flash glucose monitoring has previously been shown to reduce episodes of hypoglycaemia in patients treated with multiple daily injections of insulin whilst facilitating a concurrent trend towards HbA1c improvement [6].
In this study population, a relatively high baseline HbA1c was observed when compared to studies conducted in other countries with a similar inclusion criteria [9, 10, 15, 16]. This high baseline HbA1c reflects the difficulties in achieving adequate glycaemic control in this patient population. The COVID-19 pandemic may also have contributed to this high baseline whereby patients may have seen their healthcare professional less frequently than usual [20]. Despite the introduction of insulin, only a small proportion of people living with T2DM in the UK achieve glycaemic targets. In a retrospective cohort study of people with T2DM in primary care, only 17.3% achieved an HbA1c of < 53 mmol/mol (7%), 6 months after introducing insulin [21]. This has negative consequences for the patient as reflected by the high prevalence of complications seen in this study population, subsequently leading to increased healthcare-related costs. Based on estimates of people with T2DM not achieving glycaemic control targets, 7 years in poor glycaemic control (HbA1c 66 mmol/mol, 8.2%) increases the costs associated with diabetes-related complications by £805 million over 10 years compared with having better glycaemic control (HbA1c 53 mmol/mol, 7.0%) [22]. Flash glucose monitoring could therefore be used as an adjunct in helping such patients achieve glycaemic targets and ultimately reduce healthcare-related costs.
The present study indicates the effectiveness of flash glucose monitoring in those with a suboptimal HbA1c level. A greater decrease was observed in those with baseline HbA1c > 75 mmol/mol (9.0%), a pattern which has been confirmed by a previous meta-analysis [23]. Due to the real-world nature of this study and prescribing guidelines, it is likely that flash glucose monitoring was prescribed to those with suboptimal HbA1c levels and other factors such as recurrent or severe hypoglycaemia. The observed improvement in HbA1c is therefore most likely applicable to this population and further study is warranted to elucidate the impact of flash glucose monitoring in a wider T2DM population.
As expected, the most commonly prescribed non-insulin glucose lowering medication in this population was metformin. The prescription of GLP-1 and SGLT-2 inhibitors may have increased following data collection due to updated national guidelines for these drugs broadening their indication [8]. Baseline BMI and duration of insulin use were similar to comparable observational studies conducted in Europe [9, 10]. A significant number of patients identified in the initial search were not included into the final analysis due to a lack of HbA1c in the specified time period. Part of the data collection occurred during the COVID-19 pandemic, where pressures placed on diabetes services may have led to delays in the timely collection of routine blood tests [20].
Limitations
As a retrospective study, exclusion of patients without an HbA1c measured in the specified time periods may have generated a selection bias. Additionally, the study did not assess the impact of flash glucose monitoring in those without baseline HbA1c of 64–108 mmol/mol (8.0–12.0%). This may limit the generalisability of results to a wider population of people living with T2DM. The following information was not known for this study population: concordance with self-monitoring of blood glucose prior to commencing flash glucose monitoring, frequency of severe and non-severe hypoglycaemia, ethnicity and sociodemographic data and other CGM-based metrics (such as time in range and glucose variability). Using the same HbA1c measurement for inclusion and baseline may have rendered the analysis susceptible to a ‘regression to the mean’ phenomenon. However, the HbA1c improvement observed in this study is greater than the 0.3% decrease observed in the control group of a previously discussed RCT [11]. The absence of a control group means that the observed benefit may not be fully attributed to flash glucose monitoring. Further research is warranted to assess the reasons for the observed decrease in HbA1c including lifestyle and pharmacological changes.

Comments (0)