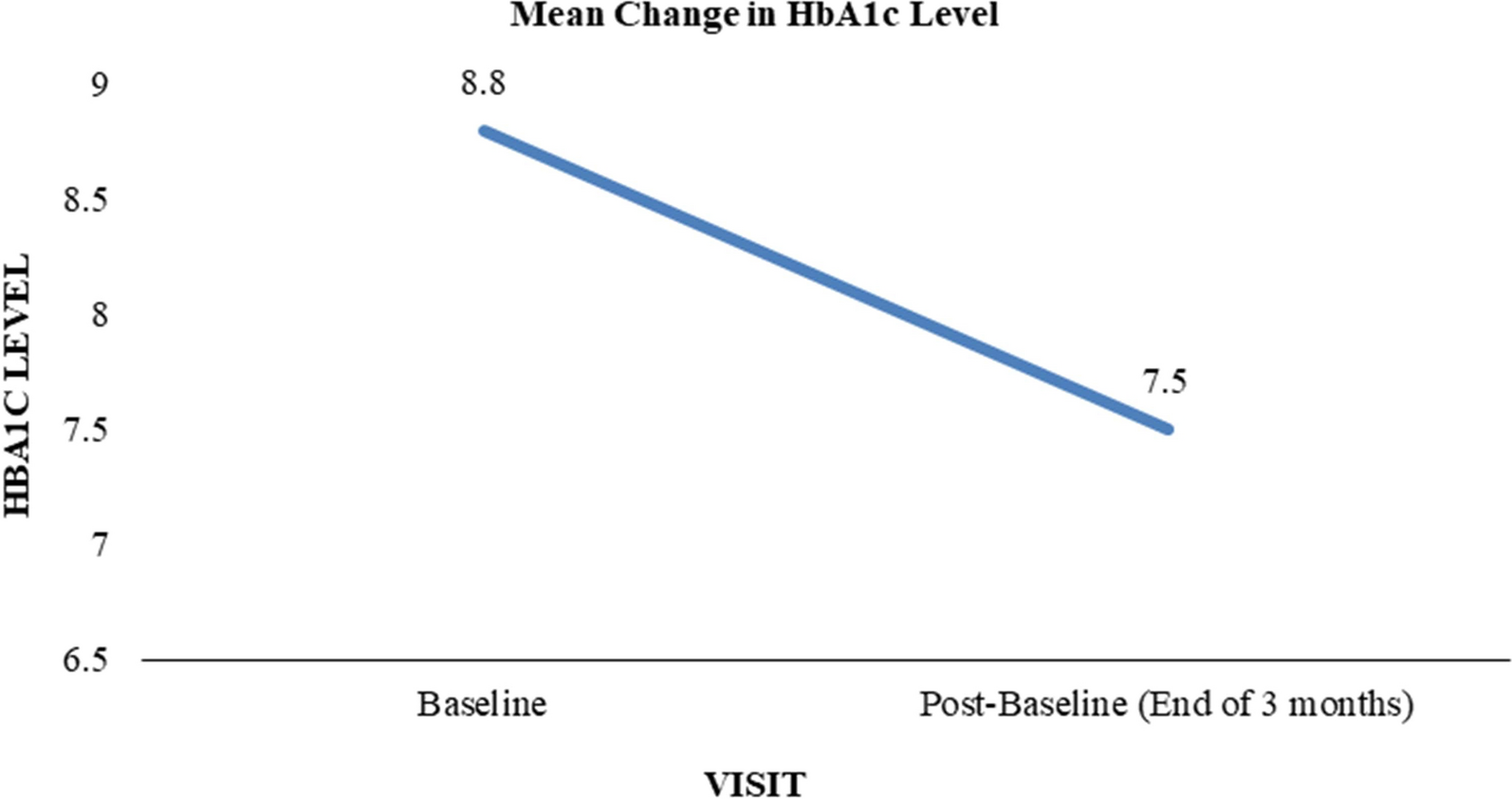
This study investigated the efficacy and safety of escalating the dose of oral semaglutide from 7 to 14 mg using real-world clinical data. Our findings indicated that escalating the dose of oral semaglutide from 7 to 14 mg in routine clinical practice resulted in notable improvements. Specifically, we observed an additional reduction of − 0.5% in HbA1c levels and a decrease of − 2.0 kg in body weight, all achieved without severe AEs. Moreover, a significant increase was observed in the proportion of patients achieving HbA1c levels < 7%, rising from 33.3% at baseline to 54.4% at 24 weeks (p < 0.01). Additionally, approximately 40% of patients achieved at least 3% weight loss compared to baseline, which is associated with beneficial effects on obesity-related risk factors and conditions according to previous findings [17]. These results align with the dose-dependent effects of oral semaglutide observed in the PIONEER clinical trials [6, 8, 12,13,14,15]. Furthermore, consistent with the results of PIONEER 8 [13], we observed a significant reduction in the total daily insulin dose from baseline. Our analysis suggests that escalating the dose of oral semaglutide to 14 mg could serve as an effective strategy for intensifying glycemic therapy and managing body weight in patients with T2D.
In the PIONEER program, the most common AEs were gastrointestinal disorders, occurring in a dose-dependent manner with oral semaglutide, requiring discontinuation in 2–12% of patients receiving 14 mg oral semaglutide [6,7,8,9,10,11,12,13,14,15]. These AEs typically manifested earlier in the study during the dose initiation and escalation phases. In the current study, gastrointestinal disorders were also the predominant AEs, occurring in 10.6% of patients. Notably, these events were more frequent in the early dose-titration group (18.2%) than in the late group (3.0%). However, these gastrointestinal disorders were mild to moderate in intensity and transient, requiring dose reduction in only one patient (1.5%), and none required discontinuation of oral semaglutide. Throughout the study period, only one case (1.5%) of blood glucose-confirmed hypoglycemia (54 mg/dL) was observed. GLP-1RAs are regarded as possessing a minimal risk of hypoglycemia owing to their mechanism of action, which is contingent on glucose levels [18]. In alignment with other GLP-1RAs, severe or blood glucose-confirmed symptomatic hypoglycemia was infrequent in the PIONEER programs, although it seemed to occur more frequently in trials combining oral semaglutide with sulfonylureas (SU) or insulin (PIONEER 3, 5, 7, and 8) [8, 10, 12, 13]. As expected, the background therapy for patients experiencing hypoglycemia in our study was SU. No cases of acute pancreatitis were reported during the study period. Overall, the AEs observed in our study were mild or moderate in severity and did not lead to drug discontinuation. These findings provide valuable reassurance for physicians hesitant to increase the dosage of oral semaglutide to the highest level because of concerns about side effects. This information can help them make informed decisions about dose escalation to achieve therapeutic benefits.
Most of the PIONEER trials indicated that oral semaglutide led to a 1–6 mmHg decrease in systolic blood pressure, and these reductions were statistically significant when comparing the effects of 14 mg oral semaglutide with those of a placebo [6,7,8,9, 12,13,14,15]. However, the present study did not show any significant changes in systolic or diastolic blood pressure. Several factors may have contributed to this inconsistency, including the limited number of patients with confirmed blood pressure changes and unspecified blood pressure measurement conditions (e.g., office vs. home measurements). Furthermore, this study investigated the effect of escalating the dose of oral semaglutide from 7 to 14 mg. Differentiating the interpretation of the effect on blood pressure from the findings of the PIONEER trial, which aimed to discern the differential effects of oral semaglutide and placebo, is important.
Non-alcoholic fatty liver disease (NAFLD) is a significant global health concern, particularly among individuals with obesity and T2D. Previous studies have highlighted the direct and indirect beneficial effects of GLP-1RAs on NAFLD, with reduced ALT and aspartate transaminase (AST) levels following semaglutide administration [19,20,21,22]. Although our study showed a tendency towards improved liver function with an escalation in the dose of oral semaglutide from 7 to 14 mg, consistent significant differences over 24 weeks were not identified.
In the PIONEER program, oral semaglutide was associated with either stable or reduced fasting lipid levels compared with other treatments, with sustained reductions over time [6,7,8,9,10,11,12,13,14,15]. Similarly, the present study indicated improvements in lipid profiles with increasing doses of oral semaglutide. However, triglyceride levels may have been influenced by dietary factors due to the lack of standardization in blood collection conditions. Further studies with larger sample sizes and controlled dietary conditions are required to elucidate the effects of oral semaglutide on lipid metabolism.
Renal function has been reported to remain unaffected during oral semaglutide treatment in the PIONEER program [6,7,8,9,10,11,12,13,14,15]. Conversely, post hoc analysis of the SUSTAIN 1–7 trials revealed initial reductions in the eGFR with semaglutide that plateaued over time, along with marked reductions in the UACR [23]. Similarly, in the present study, renal function at 12 weeks showed a slight decrease relative to baseline but did not continue to decline until 24 weeks, remaining stable at a plateau. However, no significant reduction in UACR was observed, possibly because of the small number of patients who underwent serial urinary albumin quantification, which limited adequate comparisons.
Simple regression analysis revealed a positive association between HbA1c levels at baseline and improvement in HbA1c levels at 24 weeks. This finding is consistent with previous reports indicating a greater reduction in HbA1c levels with higher baseline HbA1c levels [24, 25]. No significant interaction between the reduction in HbA1c levels and baseline BMI was observed in the subgroup analysis of the PIONEER program [24]. However, BMI at baseline was positively associated with improvements in HbA1c levels at 24 weeks in the present study. Nonetheless, this result may have been influenced by other background factors because multivariate analysis could not be performed as a result of the small number of cases. Further research is warranted to ascertain whether a higher baseline BMI is positively associated with reductions in HbA1c levels.
Avoiding clinical inertia and early intensification of diabetes therapy have been emphasized as crucial for achieving HbA1c goals [26]. In the present study, both the early and late dose-titration groups showed significant glycemic improvement, whereas only the early dose-titration group showed significant improvement in weight loss. However, the relatively short median time required for dose titration (114 days) suggests that the early dose-titration group may have been more likely to benefit from the weight loss associated with oral semaglutide initiation.
This study had some limitations. First, being a retrospective observational study conducted at a single center using historical data, the study is susceptible to confounding factors and biases. These factors may impact the results, posing challenges in ascertaining the true effects of the intervention. Additionally, it is a single-arm study without a comparator group, which limits its ability to draw direct comparisons. Although the patients were not stratified on the basis of concomitant medications, prior investigations have indicated that oral semaglutide is effective in reducing HbA1c levels and body weight, regardless of concurrent glucose-lowering agents [27]. Additionally, the constant number of glucose-lowering medications throughout the study period and the predominant reduction in the total daily insulin dose suggested a minimal likelihood of overestimating the effect of escalating the dose of oral semaglutide, validating the obtained results. However, given the potentially heightened effects of 14 mg oral semaglutide in Asian populations [24], further verification is necessary to ascertain the applicability of these results to other racial groups. AEs may have been underestimated owing to inaccurate or selective records; however, it is noteworthy that no serious AEs leading to dose reduction or discontinuation were missed owing to accurate prescription records. Second, the relatively small number of enrolled patients, although all patients prescribed 14 mg of oral semaglutide were included at the time of study planning, is a limitation. In particular, blood pressure and UACR assessments were challenging because they were often omitted or not measured. Further validation of the effects on blood pressure and UACR requires the inclusion of more cases. Third, two patients were lost to follow-up at the end of the 12-week visit as a result of hospital transfer and did not complete the full 24-week duration. Additionally, we excluded non-adherent patients, and data subsequent to the reduction or discontinuation of oral semaglutide during the observation period were not included in outcome measurements, which could introduce bias. Exclusion of non-adherent patients could lead to underreporting of adverse effects. However, only one patient was excluded because of non-adherence in this study. The patient initially switched from another GLP-1 receptor agonist to oral semaglutide but often took it after meals instead of on an empty stomach or forgot to take it altogether because of a busy morning schedule. They subsequently switched to injectable semaglutide and tolerated the maximum dosage without adverse effects, suggesting that proper oral administration would unlikely have led to adverse effects.
Future prospective studies with larger sample sizes, a comparator group continuing on 7 mg oral semaglutide, and longer follow-up durations may provide more evidence regarding the efficacy and safety of escalating the dose of oral semaglutide.

Comments (0)