
Remember me
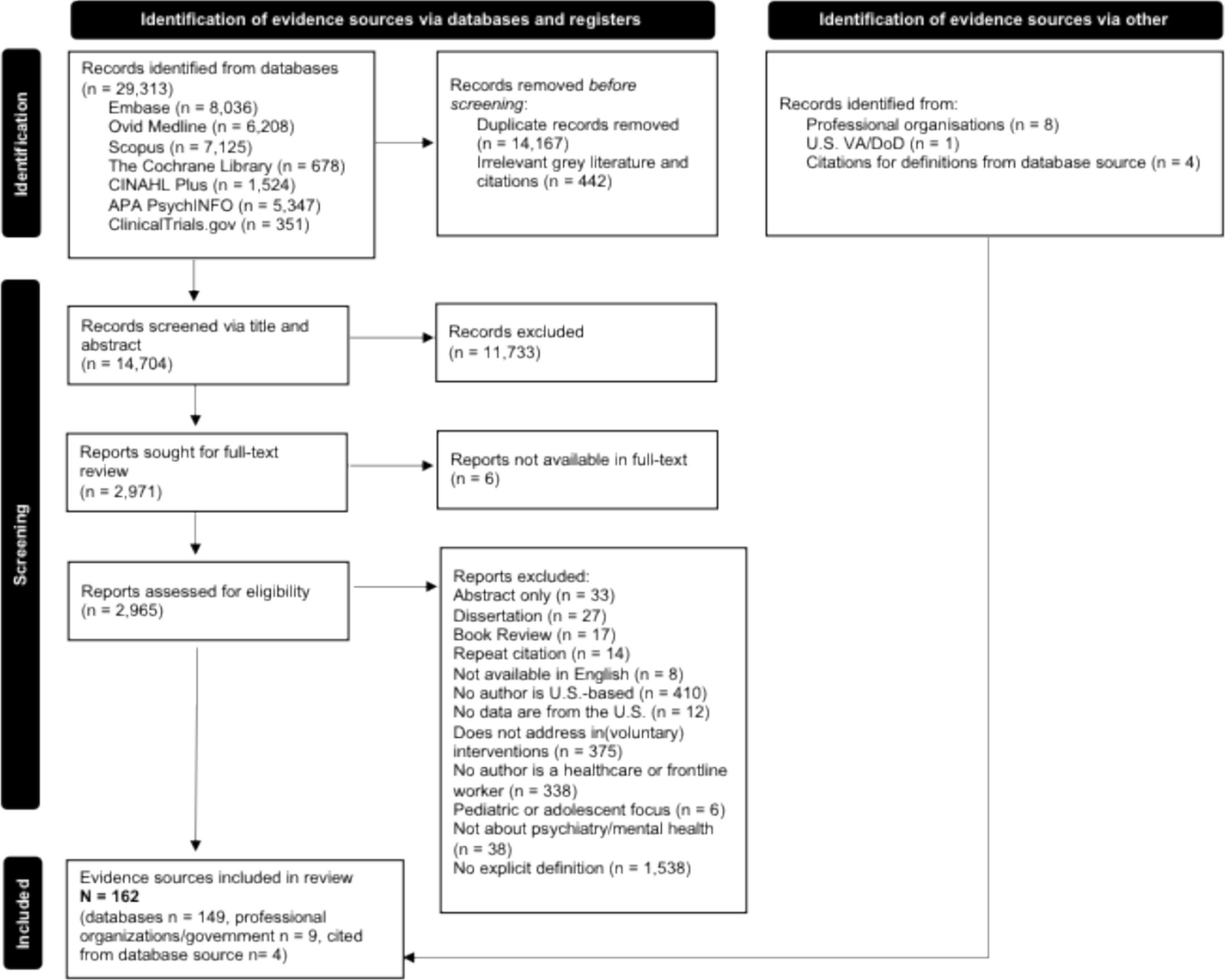




The literature search returned a total of 2611 papers. After removal of 1172 duplicates, a total of 1439 publications were screened. Following abstract and title screening as well as scanning the references of selected papers, 28 papers underwent full-text screening and data extraction, and 17 met inclusion criteria and were included in the final narrative review (Fig. 1). Of the 17 included papers, there were only 16 original studies as two papers were based upon the same study.11,12
Figure 1
Flow diagram of the study selection process. Adapted PRISMA flow diagram (2020) (http://www.prisma-statement.org/)
Study DesignThe study design of all the included studies was RCTs, ranging in duration from 4 weeks to 18 months.12,13 In all studies, the RCTs had two-arm comparisons: (1) direct comparison of TMH vs same treatment delivered in-person, (2) TMH + In-person vs In-person alone (TMH as add on to usual care), (3) TMH intervention versus in-person standard care control, and (4) TMH vs another telehealth control (such as telephone-delivered calls recalling neutral events). Six of the papers compared the same treatment delivered via TMH versus in-person interventions (35.3%).11,12, 14,15,16,17 Three papers compared an add-on TMH treatment to usual care vs usual care (17.6%).18,26,20 Five of the papers compared specific telemental health treatment to in-person control (29.4%).21,15,16,17,25 Three compared one telemental health treatment to another telehealth control, two of which were telephone-based and one video-telephone hybrid (17.6%).13,26, 27
Interventions included communication between a provider and a patient via electronic means such as telephone, videoconference, or other digital media platforms. All 17 papers used digital communication either through telephone (58.9%) or webcam/videoconferencing (41.2%). The control for the 3 studies that compared 2 TMH interventions included telephone calls recalling neutral events, adherence reminder telephone calls, or telephone-based disease management modules.13,26, 27
Descriptions of the interventions, controls, outcomes, and results are displayed in Table 2. Schulze described usual care as occasional in-person physician visits to evaluate illness compared to TMH as add-on to usual care.18 Chong used a webcam that consisted of monthly TMH visits provided by a psychiatrist using an online virtual meeting program.15 Both Lam and Schulze included components consisting of adherence-reminder telephone calls from trained nursing staff as part of their TMH intervention delivered via phone but had different comparison groups.26,18 Between the video-based and telephone-based subgroups, no outcome differences were seen (Tables 1 and 2).26,18
Table 1 Study characteristics—demographics, setting, and duration of randomized controlled trial testing telemental health interventions in patients with serious mood disordersTable 2 Interventions/outcomesSample CharacteristicsA total of 1985 participants with mood disorders were analyzed across the 17 papers. Sample age ranged from 43 to 65 years old and gender ranged from 2.5 to 100% of the participants being female. Two papers reported ages as quartiles and thus were not included in the age range.16,20 Two publications reported different outcomes on the same participants (n = 241).13,14 Baseline demographics such as age, gender, sample size, population, location, study setting, and study duration are reported in Table 1.
Fourteen of the 17 papers (82.4%) included MDD patients11,12, 14,15,16,17, 19, 20, 22,23,24,25,26,27 and four included BD patients (23.5%).13,14, 18, 21 Lastly, one article included both MDD and BD (5.9%) patients.14
Six of the papers specifically investigated TMH in rural locations (35.3%).11,15, 20, 21, 25, 27 Twelve papers were conducted in the USA (70.6%).11,12,13, 15,16,17, 19, 22,23,24,25, 27 Other represented countries included Canada (n = 2, 11.8%), Australia (n = 1, 5.9%), Germany (n = 1, 5.9%) and the Netherlands (n = 1, 5.9%).21,14, 18, 20, 26
Six of the studies were conducted in community health clinics (35.3%).11,12, 14, 15, 22, 23 Four were set in inpatient psychiatric units (23.5%).13,18, 19, 21 Three took place in primary care settings (17.6%).24,17, 27 The remainder of the studies took place at a military facility (n = 1, 5.9%), an AIDS service organization (n = 1, 5.9%), and a referral service (n = 1, 5.9%). The study duration ranged from 4 weeks to 18 months (mean = 27.9 weeks). All 17 selected papers obtained baseline data prior to implementation of the remote delivery care intervention.
OutcomesMood OutcomesAll 17 papers measured at least one clinical outcome (clinical depression, treatment response, medication adherence, patient acceptability, etc.). The majority of the papers (n = 12) had a primary outcome of change in mood symptoms among the following groups: TMH compared to in-person care alone, and the same treatment delivered via TMH and in-person. In the same intervention delivered via telehealth vs in-person comparison group, Chong found that while depression scores decreased more rapidly among treatment delivered via a video webcam vs in-person treatment group, there was no statistically significant difference in the depression score between the two groups.15 Luxton reported relatively strong and similar reductions in depression symptoms, hopelessness, and PTSD symptoms across both traditional office and videoconferencing groups comparing the same intervention.16 Egede found no significant differences between in-person treatment CBT compared with tCBT trajectories over time on the self-reported Beck Depression Inventory (BDI) and Geriatric Depression Scales (GDS).11,12
Two papers focused on telephone-administered cognitive behavioral therapy (tCBT) compared to in-person CBT control.22,23 Fann et al. found significant improvement on the patient-reported symptom checklist and greater satisfaction with depression care compared to the in-person group p < 0.001; however, there were no differences in clinician-rated Hamilton Depression Rating Scale (HAM-D) scores between the groups.22 Mohr did not find any significant difference in depression outcomes as measured by the clinician-rated HAM-D between patients receiving in-person treatment versus patients receiving tCBT.23
Three papers observed TMH treatment added on to usual care versus in-person usual care. Dobkin reported significant self-reported improvements in mood with tCBT compared to treatment as usual (TAU) which was defined by psychiatric consultations, medication management, supportive psychotherapy, and all aspects of routine care.19 Dennis examined clinical depression outcomes in post-partum patients between TMH interpersonal psychotherapy (IPT) plus in-person treatment versus in-person treatment alone.20 In this article, Dennis found that patients treated with both IPT and standard care were 4.5 times less likely to be clinically depressed than individuals in the standard local postpartum care group.20
Three papers examined mood outcomes in TMH vs telehealth control groups. Celano found improved positive affect, as measured by the Positive and Negative Affect Schedule (PANAS), as well as improved optimism and significant reductions in hopelessness, as measured by a five-point Likert scale, in the telephone-delivered positive psychology group compared to patients receiving telephone calls recalling neutral events.13 Lam et al. did not find a significant difference in depression change scores based on the Montgomery–Åsberg Depression Rating Scale (MADRS) after 12 weeks between patients who received escitalopram + tCBT vs those who received escitalopram + control telephone-based medication reminders.26 Hilty found clinical improvement for depression in both groups that received either telephone-based intensive disease management modules (IDMM) and televideo-based psychiatric consultation versus telephone-based disease management (DMM) alone with a significant trend favoring the IDMM group.27
Medication AdherenceIn three papers, medication adherence was a reported outcome. D’Souza reported increased treatment adherence, which resulted in fewer readmissions and relapses, when comparing inpatients who received team-based videoconference discharge planning and six telemedicine-based psycho-educational program sessions, compared to inpatients who received in-person discharge summaries and no psycho-educational program.21 In another study, Schulze found that patients who received regular telephone calls as stand-alone therapy from specially trained nurses were significantly more likely to be adherent to their medications at 6 months, according to the Medication Adherence Report Scale (MARS), compared to patients who only had intermittent in-person visits with a physician with no TMH intervention.18
Finally, Kalapatapu reported that in-person CBT care and tCBT did not significantly differ in the number of CBT sessions attended, treatment engagement, treatment completion, or discontinuation of treatment.17
Patient Satisfaction and Study AttritionPatient satisfaction was a reported outcome in several included papers. Hulsbosch used the Geestelijke Gezondheidszorg (GGZ) Thermometer, a personalized patient satisfaction questionnaire, and found that videoconferencing compared to control in-person usual care had a positive effect on patient satisfaction.14 However, no significant difference was found between the two groups on quality of life, loneliness, daily functioning, or the fulfillment of needs of care.14 Similarly, Mohr reported that patients were significantly more satisfied with a 20-week program for depression using tCBT compared to treatment as usual.
Comments (0)