
Remember me
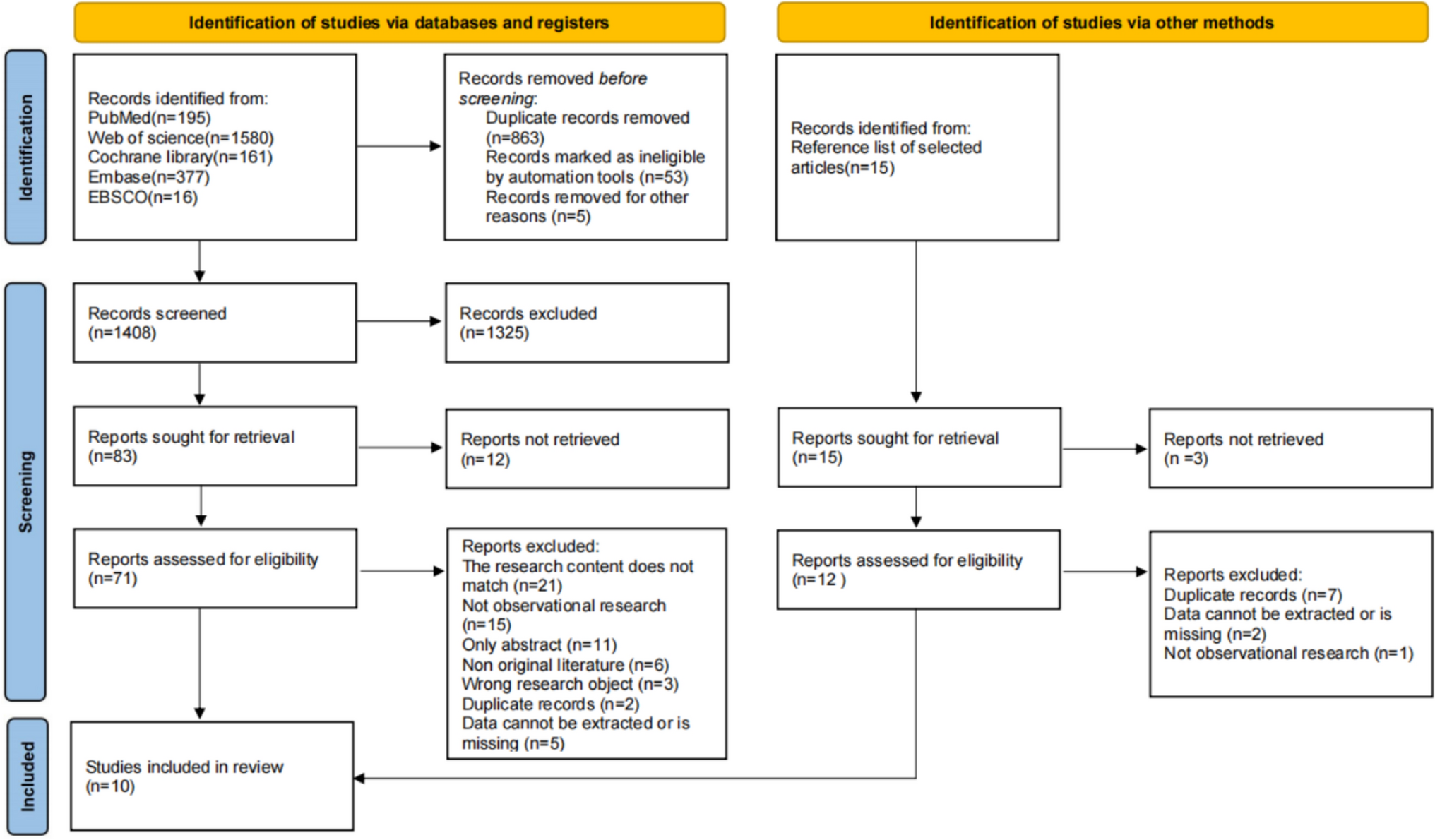
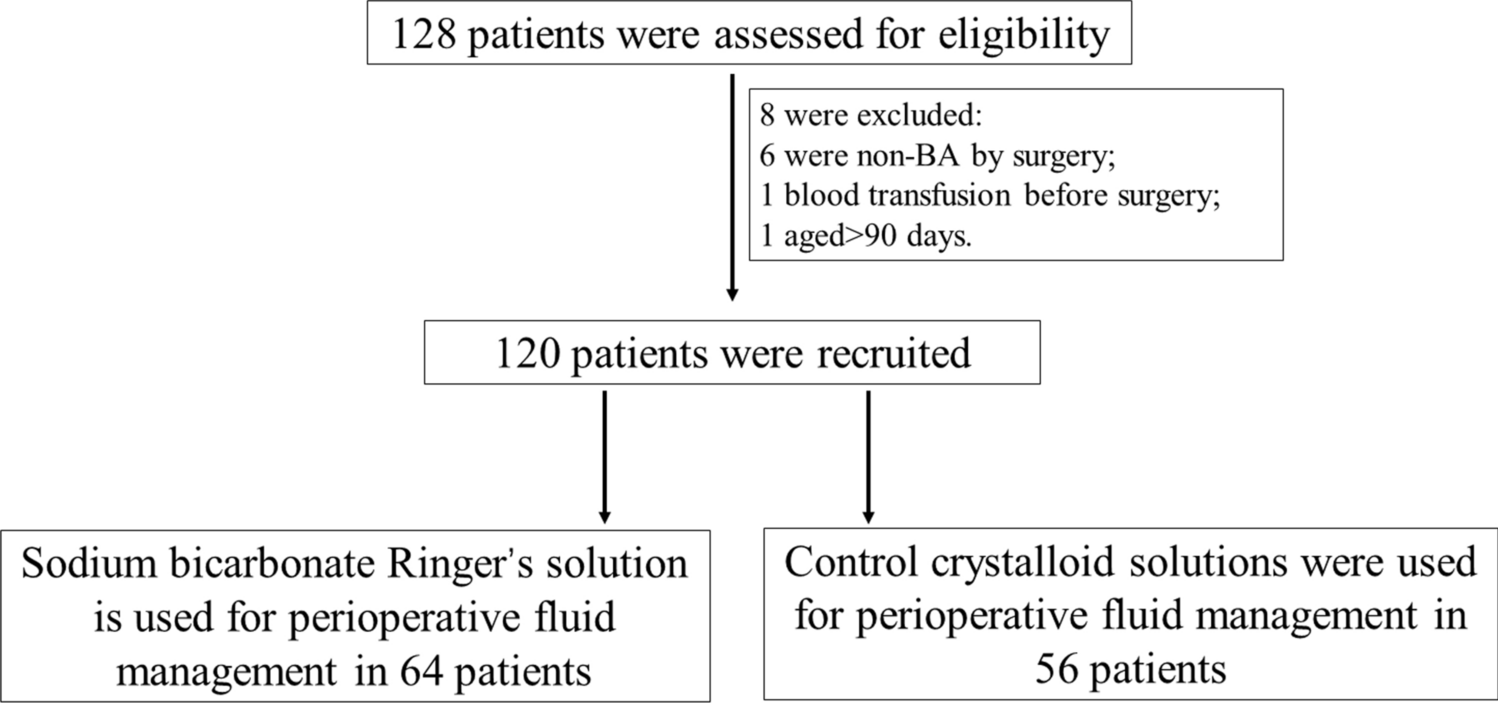


An initial review of inpatient admission records and records from the colorectal OPD identified 17 patients with rectovaginal fistulae as potential participants to the study. Seven patients were subsequently removed based on exclusion criteria, leading to study population of ten patients (n = 10) (Fig. 1). Treatment trajectories for included patients are summarised in Table 1.
Fig. 1
Patient selection flowchart
Table 1 Overview of treatment trajectories for HIV-associated RVF (patients ordered by date of birth)Patient characteristics at presentationAll patients in the study had confirmed HIV infection. Six patients (6/10) were diagnosed by PCR and four (4/10) by ELISA. Patients were diagnosed with HIV at a median age of 10 months (IQR: 1 month to 2 years 3 months). All patients were initiated on HAART in accordance with South African guidelines on management of HIV in paediatric patients [22].
Acquired RVF was a presenting feature of HIV disease for four (4/10) patients—one patient developed an RVF in their first year of life but was only formally diagnosed with HIV at the age of 2 years. The remaining 6/10 patients presented with an acquired RVF a median of 14.5 months (IQR: 10–23 months) following their HIV diagnosis.
The median age of presentation with RVF across all included patients was 2 years (IQR: 1–3 years). The youngest and oldest ages of presentation were 6 months and 7 years 4 months, respectively. Seven (7/10) patients presented with vaginal passage of stool and three (3/10) with perineal sepsis. Eight patients (8/10) were managed at CHBAH throughout their treatment period, while two patients underwent part of their treatment at other institutions.
Patients’ median HIV viral load at presentation with RVF was 19,622 copies/ml (IQR: undetectable to 1,227,558 copies/ml). Six patients (6/10) presented with an unsuppressed viral load. Viral load at presentation was suppressed (< 1000 copies/ml) in one patient (1/10) and undetectable (< 100 copies/l) in 3/10 patients. Patients’ median CD4 count at presentation was 524 cells/μl (IQR: 362 cells/μl to 1024 cells/μl). Based on their ages, CD4 counts, and comorbidities at presentation, one patient (1/10) was classified as having stage 1 HIV disease (low risk), while 9/10 patients were classified as having stage 3 disease (AIDS). Of note, the three patients who presented with an undetectable viral load were still classified as having stage 3 disease due to previous history of AIDS-defining illnesses, which included HIV encephalopathy, extrapulmonary tuberculosis, and CMV colitis (see Appendix 1).
Surgical managementNine patients (9/10) underwent surgical management of their RVF. One patient presented at the age of 6 months with multiple issues including fungal sepsis, encephalopathy, and vaginal passage of stool. Colostomy was not attempted in the index admission as the patient was judged too unwell to undergo surgery. The patient improved and was discharged but later developed chronic pulmonary disease requiring readmission. She demised from bronchopneumonia at the age of 10 months before any surgical management could be initiated.
A total of 82 procedures were performed for the patients who underwent surgical management. The median number of required surgeries per patient was of 7 procedures (IQR: 4.5–12.5 procedures) (Table 2). All patients underwent a diverting colostomy prior to RVF repair. None of the patients showed spontaneous RVF resolution following faecal diversion. Seven patients (7/9) had their stoma permanently reversed, while two patients (2/9) have long-term stomas.
Table 2 Surgical procedures performed for patients with HIV-associated RVF, according to recurrenceFistula repair was performed a median of 17 months (IQR: 7.5–55 months) following colostomy, whereas definitive stoma reversal was performed a median of 16 months (IQR: 3–25 months) after initial fistula repair. Patients whose RVF recurred after the initial repair required 9.3 additional procedures (95% CI 1.9–16.6 procedures, p = 0.02) and had their stoma reversed 19.5 months later (95% CI 2.6–36.4 months, p = 0.03) compared to patients who did not experience recurrences. No significant difference in number of surgeries required or time from fistula repair to stoma reversal was observed based on patients’ history of complications such as anal stenosis or sepsis.
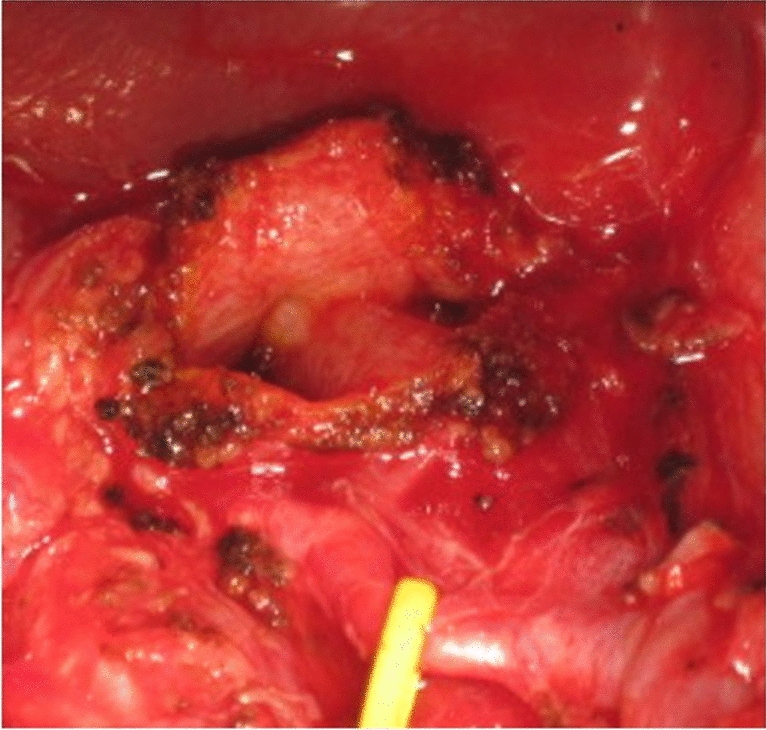
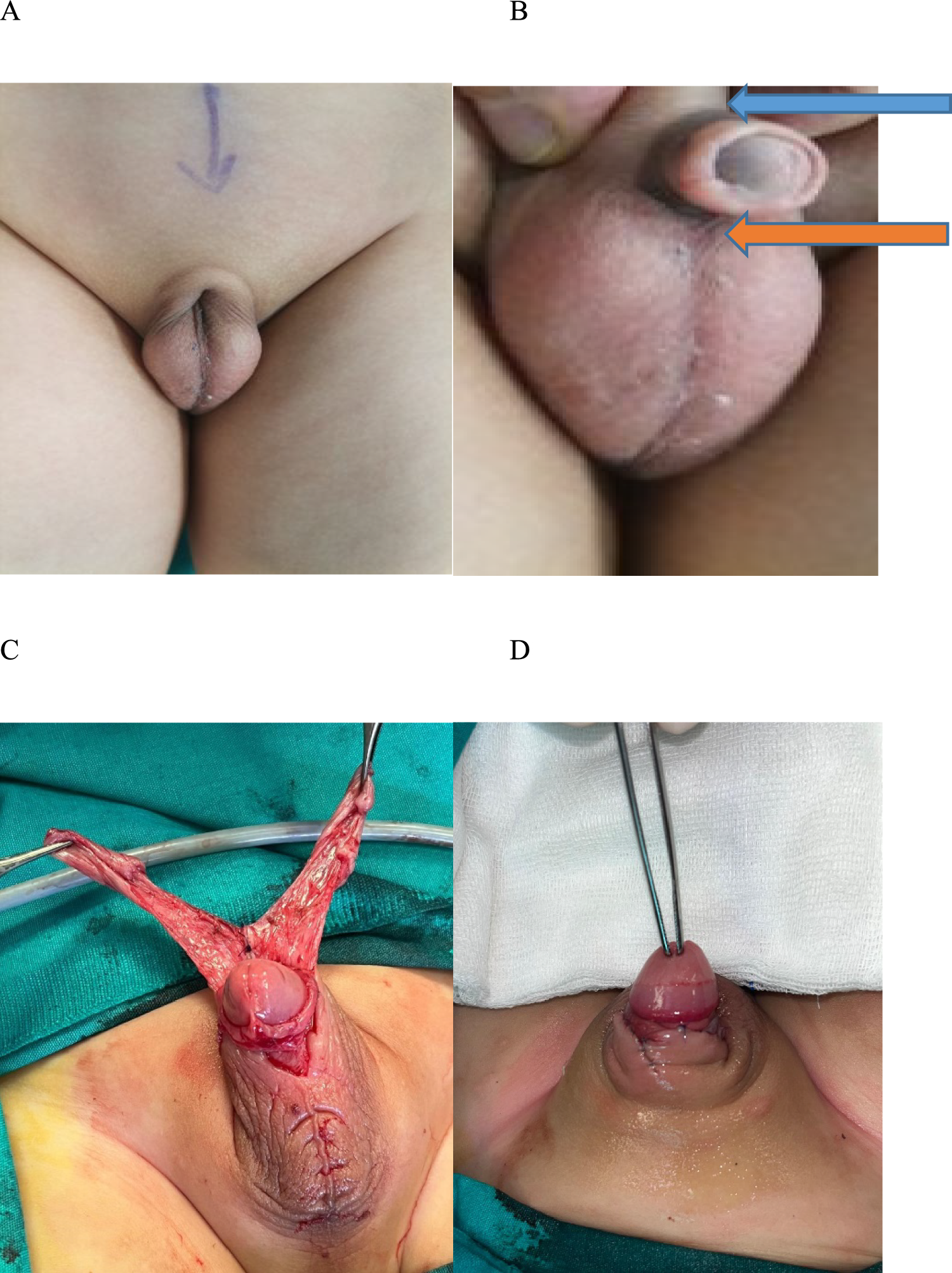
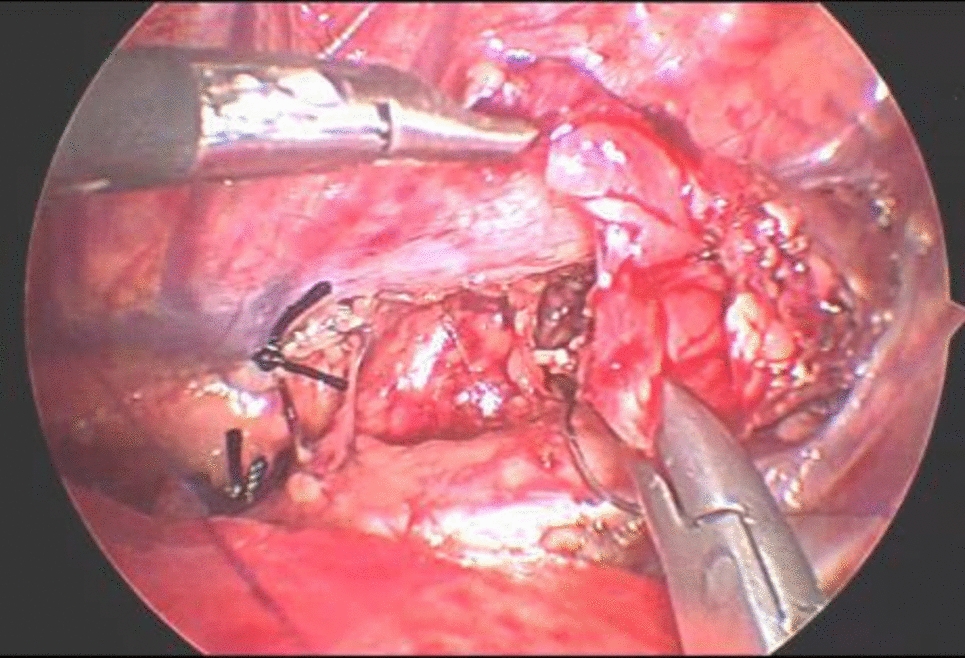
A posterior sagittal anorectoplasty was performed to repair the RVF for the first two patients in the study. Fistula repair in all subsequent patients was performed by a transanal anterior rectal wall pull-through, leaving the perineal body intact. After inserting a Lone Star® retractor at the mucocutaneous junction, the fistula is identified and the mucosal lining is debrided. Stay sutures are placed on the anterior wall of the rectum proximally to the fistula. Using needle-tip diathermy, an incision is made distal to the stay sutures and deepened. The fistula is closed with interrupted absorbable sutures. The anterior rectal wall is then pulled through using an endorectal advancement flap to cover the repair [23]. An ischiorectal fat pad can be interposed between the fistula repair and the anterior rectal wall before the anastomosis is performed (Fig. 2). An ischiorectal fat pad was interposed in the initial fistula repair for five (5/9) of our patients. Fat pad interposition in the initial repair was not observed to have a significant association with risk of subsequent recurrence. A fat pad was always interposed in procedures for the repair of recurrent fistulae [24].
Fig. 2
Steps to transanal RVF repair. a Insertion of Lone Star® retractor and fistula visualisation. b Placement of stay sutures on the anterior rectal wall. c Mobilisation of the anterior rectal wall. d Closure of the fistula tract. e Ischiorectal fat pad interposition. f Advancement flap pull-through and anastomosis
Patients only underwent fistula repair once their viral load had been suppressed (Table 3). Patients’ median viral load at the point of fistula repair was undetectable (IQR: undetectable to 217 cells/ml) and their median CD4 count was 1395 cells/μl (IQR: 978 cells/μl to 1824.5 cells/μl). No significant difference in viral loads and CD4 counts at presentation and at fistula repair was observed based on patients’ later history of recurrence or complications.
Table 3 HIV treatment trajectories in patients with surgically managed RVFComplications and outcomesThe most common complications in our patients were recurrence of the fistula, anal stenosis, and wound or perineal sepsis. Four patients (4/9) had RVF recurrences, which were observed a median of 5 months (IQR: 4–6 months) after the preceding repair. Two patients had a single recurrence and two patients had two recurrences, for a total of six recurrences. Three recurrent fistulae were repaired by re-do pull-though with ischiorectal fat pad interposition. In the other three cases, recurrent fistulae were associated with perineal disruption and damage to the anal sphincters. Fistula repair was therefore combined with perineal body reconstruction through a posterior sagittal approach. Overall, 15 procedures for RVF repair were performed.
Two patients (2/9) developed stenosis of the anal canal as a complication of fistula repair. Anal stenosis was satisfactorily managed with serial anal dilatations in one of the patients, while the other patient developed a long-standing anal stricture and was subsequently lost to follow-up.
Sepsis was observed in 3/9 patients. Two patients developed perineal sepsis due to wound dehiscence following fistula repair, while one patient developed both perineal sepsis following fistula repair and laparotomy wound sepsis as a complication of stoma revision.
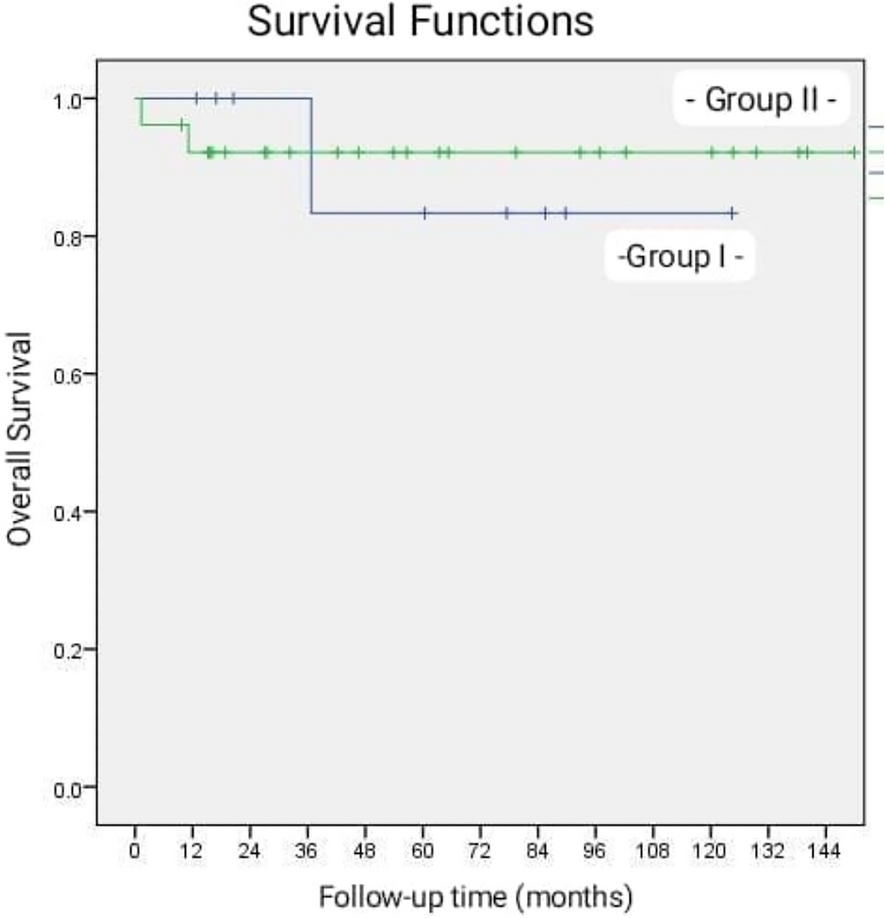
Patients were followed up for a median of 34 months (IQR: 14–84 months) after their last repair procedure. Three patients (3/9) attended in-person follow-up during the study period and three patients (3/9) were contacted telephonically. The remaining 3/9 patients could not be contacted and were classified as lost to follow-up. Information on their functional outcomes was obtained from the last available clinic note. Seven patients (7/9) have had good long-term outcomes, defined as stoma reversal and continence without any soiling episodes. Specifically, three patients (3/9) have remained continent since stoma reversal with no soiling, while four patients (4/9) experienced soiling episodes relating to constipation. These were treated with courses of bowel management with rectal washouts and laxatives: three patients have remained continent after discontinuation of bowel management, while one patient is clean on long-term daily rectal washouts. One patient is also on long-term topical treatments, having suffered extensive perineal excoriation due to sepsis.
Two patients (2/9) have long-term stomas and were classified as poor functional outcomes. The first patient had multiple complications, including recurrence, anal stenosis, and perineal sepsis. Colostomy reversal was performed with a covering ileostomy due to a short inflamed rectal stump. The patient was discharged, but represented the following month with symptoms of bowel obstruction which required an emergency laparotomy. Following multiple relooks, a colectomy and a long-term ileostomy were performed. The patient currently has extensive damage to the anal sphincters and disruption of the dentate line due to previous perineal sepsis and was thus judged unsuitable for stoma reversal. In the second patient, colostomy reversal was performed after a recurrent RVF was repaired by re-do pull-through. After 4 months, she represented with a second recurrence and a colostomy was refashioned. Re-do fistula repair and perineal body reconstruction were performed but were later complicated by development of a persistent anal stricture. This was being managed by serial anal dilatations, but the patient was subsequently lost to follow-up before her stoma could be reversed.
Patient’s surgical outcomes were not observed to significantly correlate to their HIV status at presentation. Patients who presented with an unsuppressed viral load did not differ from patients who presented with a suppressed viral load in overall number of surgical procedures, delays to fistula repair and stoma reversal, rate of recurrence or complications, and functional outcomes. By contrast, post-operative maintenance of viral control was significantly associated with surgical outcomes. Five patients (5/9) maintained a suppressed viral load following fistula repair, while four patients (4/9) were noted to have an unsuppressed viral load at some point after repair (Table 1). Failures in viral suppression occurred a median of 12.5 months (IQR: 7–16 months) after the previous repair. Compared to patients who maintained viral suppression after fistula repair, patients who experienced post-operative failures of viral suppression were noted to have a significantly higher rate of recurrence or complications including anal stenosis and sepsis (Table 4).
Table 4 Viral suppression and surgical outcomes (fistula recurrence, anal stenosis, or sepsis)
Comments (0)