
Remember me
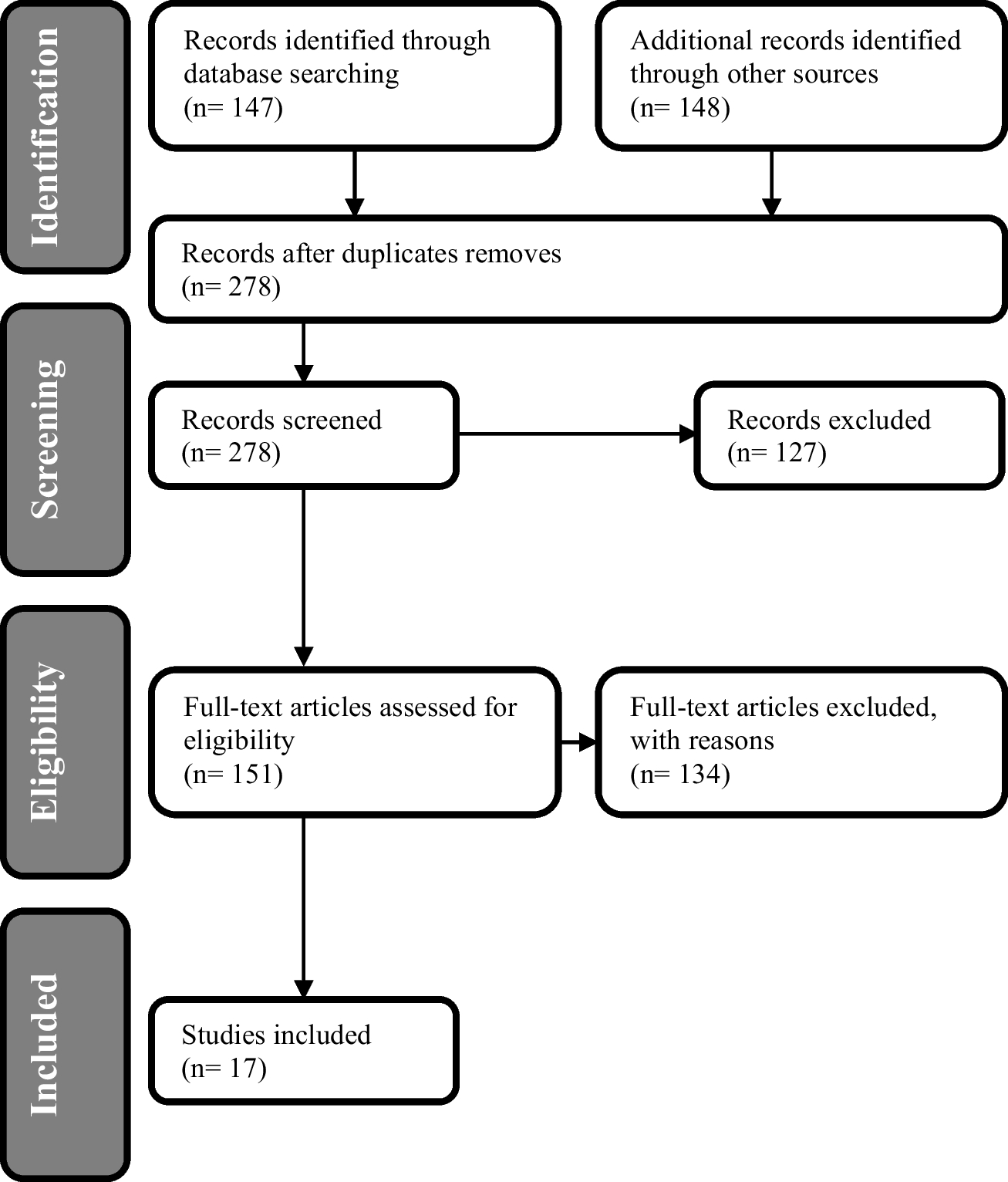

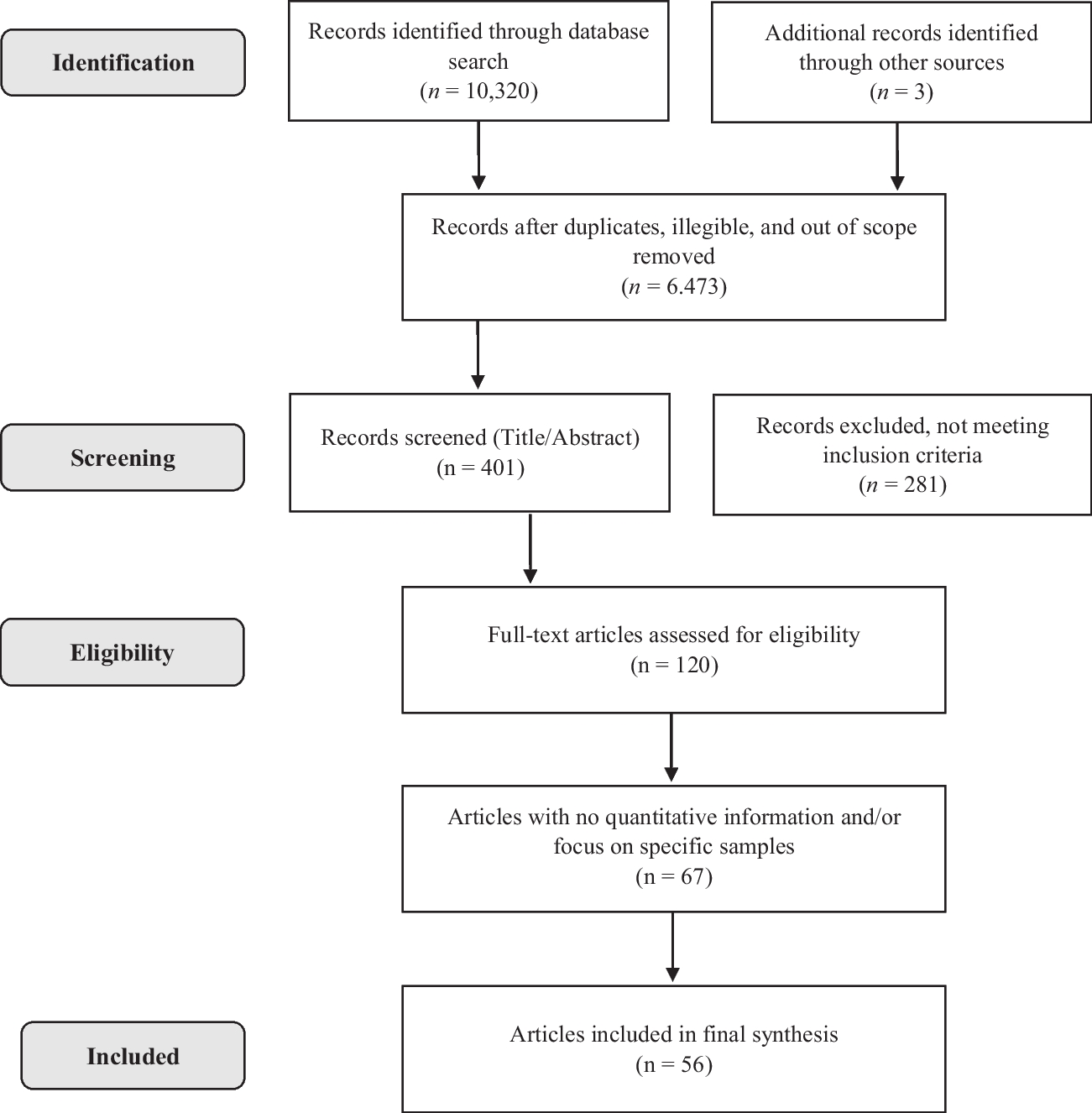
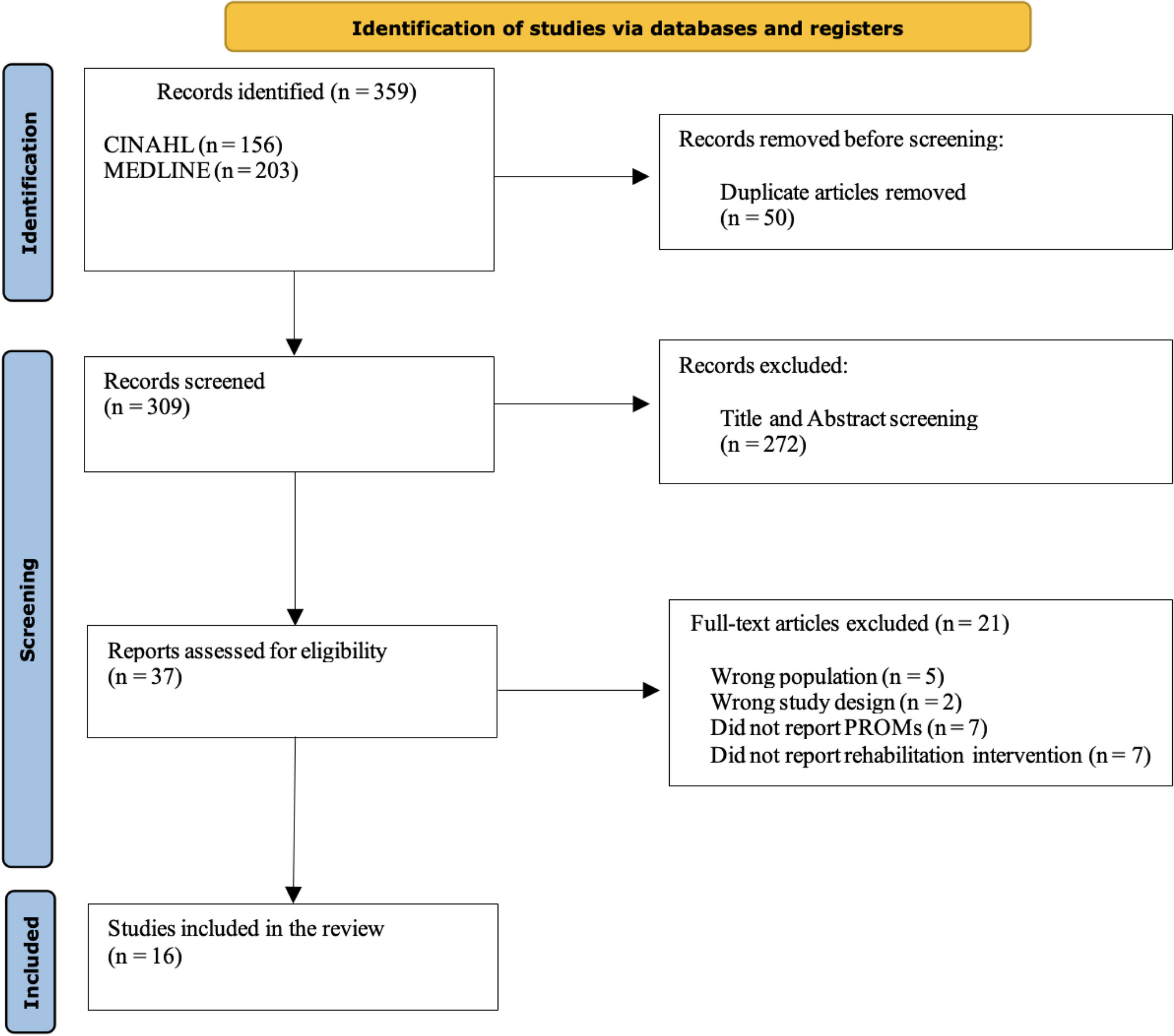
Of the 2823 references from the queried databases, removal of duplicates resulted in 206 articles being screened, which, following exclusion by title and abstract led to the reading of 23 full texts, resulting in the final inclusion of eight papers that met the inclusion criteria (Fig. 1).
Fig. 1
The papers included were published over a rather brief span of time between 2003 and 2021. Three of them (Halbach et al. 2020; Hiltrop et al.2021; Midding et al. 2018) are part of the German N-MALE project study (Male breast cancer: patient’s needs in prevention, diagnosis, treatment, rehabilitation and follow-up-care), which was started in April 2016 and which ended in March 2018. The intention of the programme was to identify the prevention, diagnosis, treatment, rehabilitation and follow-up needs of men with breast cancer. In “Men with a ‘Woman’s Disease’: Stigmatization of Male Breast Cancer Patients—A Mixed Method Analysis” (Midding et al. 2018) the feminisation of breast cancer was described. The authors used a mixed method to collect qualitative interviews (n = 27) and quantitative data (n = 100). These data tended to highlight the theme of stigmatisation and ignorance regarding male breast cancer mainly in cancer care settings and in the workplace, where men reported that they had the feeling of being isolated from colleagues and projects. In the healthcare system, male breast cancer patients (MBCPs) reported that they felt unwelcome and awkward while intruding in an area normally reserved for women.
The second article derived from the N-MALE project (Halbach et al. 2020) focused on exploring the health situation of MBCPs from their own perspective. The sample and method used were the same as those described in Midding et al. (2018). Positive experiences emerged, alongside findings of shortcomings such as delays in diagnosis, uncertainty of health professionals about treatment, experiences of stigmatisation and problems with continuity of care, including unclear responsibilities for aftercare and difficulties in accessing specific breast cancer care for men in a gynaecological context.
Also within the same N-MALE project, Hiltrop’s (Hiltrop et al. 2021) paper involved the sample of 27 participants described in Midding et al. (2018) with the aim of exploring the MBCPs’ experiences of returning to work and in particular of answering questions regarding the type of return-to-work patterns among them. This included the MBCPs’ reported motivations to return to work, how they experienced their return to work and how their illness affected their work after they had returned. Among the motivations that emerged for returning to work were the desires for normality and for diversion, the need to stay active and to maintain social contacts. They also viewed work as a source of pleasure, along with its economic motivations, whilst the lack of perception of being ill and the possibility of having a job that requires little physical effort were also deemed significant. Participants reported a positive workplace experience throughout the period of illness right up through their return to their jobs, although they did emphasise that there was a perceived experience of stigmatisation. The consequences of the illness and treatment led to changes in the respondents’ productivity, e.g. due to fatigue.
The aim of Nguyen’s German paper (Nguyen et al. 2020) was to explore the experiences of men with breast cancer by identifying their needs for care and support. The interviews, which involved a group of 18 MBC patients, revealed a largely neutral experience of being affected by this “women’s disease”, although some felt that stigmatisation did threaten their masculinity. They reported the perception that being male appeared to be an obstacle to accessing adequate care. In fact they identified key barriers to their care options, including lack of awareness and experience in treating men for BC among health professionals, as well as the perception that all breast cancer research was based on female populations and that there was a lack of dedicated support services for MBCPs.
Williams’ paper (Williams et al. 2003) was aimed at exploring the experiences of men in England who had been diagnosed with breast cancer and comparing them with those of women with the same disease and the experiences of health professionals caring for both groups of patients. A series of four focus groups was conducted, and the groups included men with cancer, women with breast cancer and a group of healthcare professionals (breast surgeons, nurses and oncologists) with a total of 27 people. The men reported that they went to their doctor because of their partner’s insistence. Most men indicated that they would appreciate the opportunity to talk to another man with breast cancer. Iredale’s paper (Iredale et al. 2007) was also conducted in England through multi-stage research. Most of the men surveyed were shocked to receive the diagnosis of breast cancer, whilst sharing that diagnosis resulted in embarrassment and stigma. In this paper, too, there emerged the issue that only limited information on MBC was available. What was available was often viewed as inappropriate as it was originally intended for women. The study conducted in the USA (Walker and Berry 2020), part of a longer paper, analysed the experiences of five men. Once again, their reporting revealed the total inadequacy of their having to be cared for in treatment spaces dedicated to women.
Most recently, the Israeli paper (Levin-Dagan and Baum 2021) involved 16 men. Interestingly, the results showed that the participants faced stigmatising situations both inside and outside healthcare facilities. These men’s coping styles showed situational responses wherein they used disengagement, such as concealment and selective disclosure, with the aim of destigmatising their being affected by MBC.
Comments (0)