
Remember me

In Italy, the public health system offers mammography screening every two years for women aged 50–69 years. Conversely, only a few regions, notably Emilia-Romagna, have implemented annual mammography screening for women aged 45–49 years [37, 38]. In contrast, the Veneto Region, like most Italian regions, does not yet have a mammography screening programme for women aged 45–49 years, despite the fact that breast cancer incidence rates are comparable to those observed among women aged 50–54 years [39, 40].
In 2018, the Veneto Institute of Oncology (IOV) addressed this gap by proposing a project to the Veneto Region, aiming to explore the feasibility and sustainability of a personalized screening programme. This innovative approach incorporates tomosynthesis, individual breast density, and risk estimation to personalize screening of women aged 45–49 years. The Regional Administration approved a feasibility study focusing on 45-year-old women residing in the provinces of Padua and Rovigo, totaling about 10,000 women per year. Given the limited pool of eligible participants, a quasi-experimental approach was adopted. In this setup, IOV formed the prospective cohort, while the observational control cohort was enrolled from the Emilia-Romagna Region.
Study designThe study uses a quasi-experimental design of pre-post comparison with a non-equivalent control group [41]. Quasi-experimental designs, wich are used when random intervention assignment is impractical or unethical, reflect real-world conditions and allow for generalization. Despite practicality, cost-effectiveness, and higher external validity, this design may suffer from lower internal validity due to systematic differences between interventional and control groups. Nonetheless, non-experimental designs have been already used to assess the impact of public health mammography screening on the incidence of advanced breast cancer [42, 43].
We recruited a prospective interventional screening cohort of 45-year-old women from two provinces of the Veneto Region. These women, after initial screening, were divided into five subgroups based on their breast density and individual risk and were referred for different screening intervals and imaging protocols until the age of 49 years. At the same time, we assembled an observational cohort from the Emilia-Romagna Region, composed of women of the same age who underwent standard annual mammography screening. This population will serve as a nonequivalent control for comparative purposes.
The study hypothesis is that a screening model stratified by breast density and risk is more effective and sustainable in reducing the incidence of advanced breast cancer than standard annual mammography screening.
Both the interventional and control cohorts are studied using a two-phase design involving a pre-screening period followed by a screening period. The pre-screening phase measures the baseline incidence rate of breast cancer in women aged 45–49 years in both populations. This baseline assessment helps calculate the ratio of the incidence rate at baseline between the Veneto Region and the Emilia-Romagna Region for subsequent statistical adjustment. During the screening period, the two screening models are implemented, and cumulative incidence rates of advanced breast cancer are assessed over 3 years, 5 years and 10 years (at least). The ratio of the cumulative incidence rate in the interventional cohort to that found in the observational control cohort, adjusted for differences in incidence at baseline, is calculated. The decision to evaluate the results at three-year intervals stems from previous research that demonstrated a significant decline in the incidence of pT2-4 stage breast cancer from the third year of screening [44]. The extended follow-up duration takes into account the potential lasting preventive impact of screening beyond age 50 and incorporates the common biennial digital mammography screening procedure for women over age 50.
Interventional cohortThe prospective interventional cohort consists of women aged 45 years from two provinces in the Veneto Region. The enrollment phase for this cohort has been completed, with a final number of participants of 10,269 women. Participants initially met specific criteria and are now undergoing successive screening rounds with different intervals and imaging protocols until the age of 50.
During the initial screening round, participants underwent two-view digital breast tomosynthesis (DBT) of both breasts. They also completed a questionnaire on risk factors such as personal characteristics, hormonal factors, family history of breast cancer, lifestyle, and health status. Volumetric breast density (VBD) values were calculated with Volpara software from DBT images [45]. Subsequently, women with an average VBD greater than 25% were invited for supplemental ultrasound (US). Based on individual risk factors and mean VBD, we used the Tyrer-Cuzick risk model to estimate lifetime risk (LTR) for each woman [17, 22]. This risk assessment categorized women into five subgroups each recommended for a personalized screening protocol:
1.Low-Risk, Nondense Breasts: Women with LTR ≤ 17% and VBD < 25% are recommended for biennial DBT screening;
2.Low-Risk, Dense Breasts: Women with LTR ≤ 17% and VBD ≥ 25% are recommended for biennial DBT screening with supplemental US (DBT + US protocol);
3.Intermediate-Risk, Nondense Breasts: Women with LTR between 17 and 30%, or LTR > 30% without family history, and VBD < 25% are recommended for annual DBT screening;
4.Intermediate-Risk, Dense Breasts: Women with LTR between 17 and 30%, or LTR > 30% without family history, and VBD ≥ 25% are recommended for annual DBT + US screening;
5.High-Risk, Any Breast Density: Women with LTR > 30% and a family history of breast cancer, are recommended for annual DBT and magnetic resonance imaging (MRI) surveillance, regardless of breast density.
These individualized recommendations based on density and risk offer personalized screening protocols. For low to intermediate risk nondense breasts, DBT examinations were/are performed during initial and subsequent rounds and interpreted independently by two breast radiologists. For dense breasts at low or intermediate risk, DBT and US are performed by a single breast radiologist. Abnormal findings require further evaluation, including additional imaging and, if necessary, biopsy. Post-treatment follow-up plans are initiated for confirmed breast cancer cases. Informed consent was obtained by all women participating in the interventional cohort.
Observational control cohortBetween 1995 and 1997, the Emilia-Romagna Region started a double-reading mammography screening programme for women aged 50–69 years, which switched from analog to digital mammography (DM) in 2010–2011. The programme was extended to women aged 45–49 years and 70–74 years in 2010, with an annual screening interval for the younger age group [46]. In the context of the RIBBS study, the observational control cohort includes women 45 years of age residing in three provinces of the Emilia-Romagna Region. These individuals participated in the annual screening programme from 2012 to 2020.
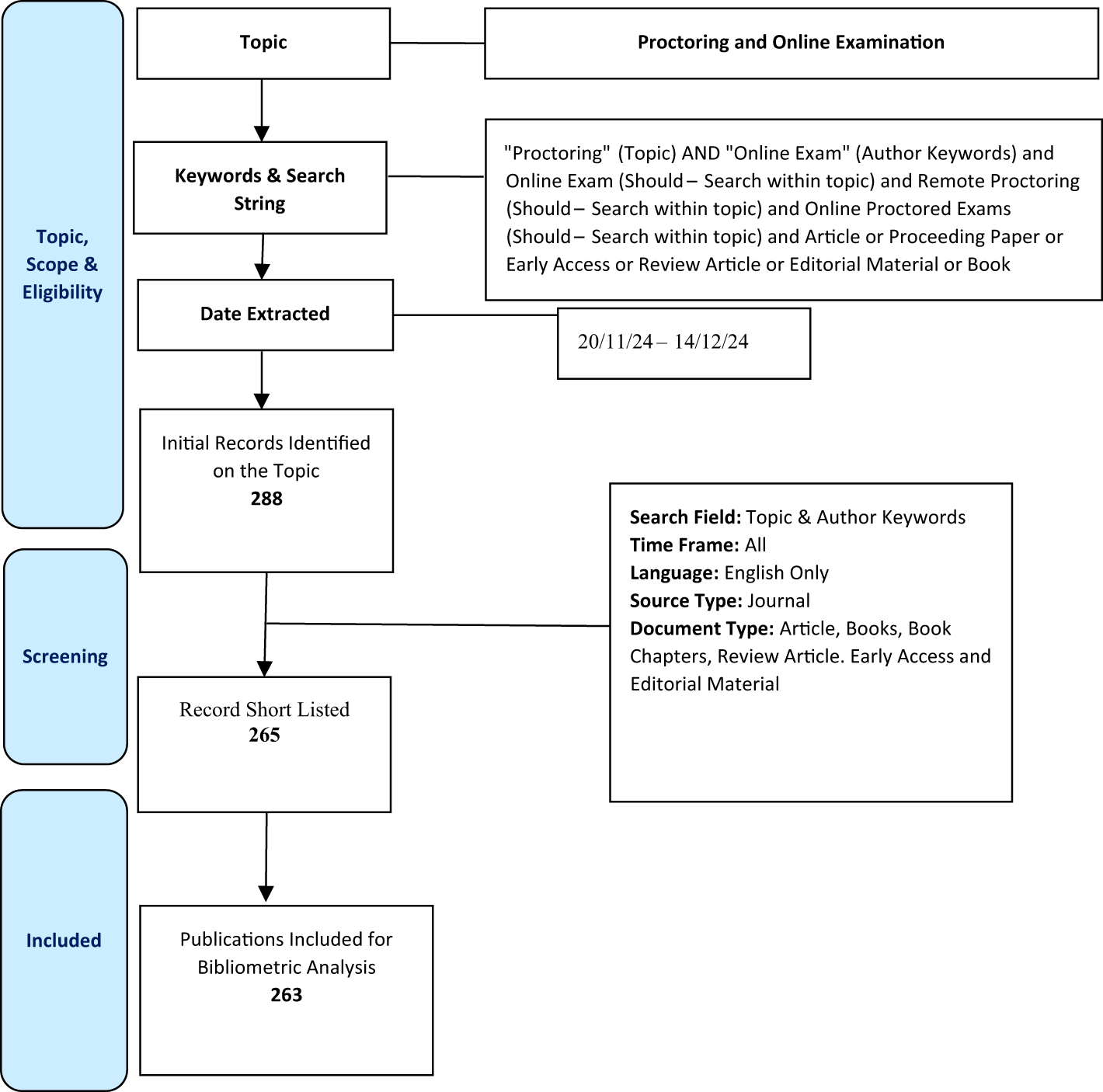
The five subgroups of the interventional cohort and the observational control cohort are depicted in Fig. 1.
Fig. 1
Technical scheme depicting the five subgroups of the interventional cohort and the observational control cohort of the Risk-Based Breast Screening (RIBBS) study
Pre-screening and screening periodsThe pre-screening phase for the interventional cohort ran from 2017 to 2019, while that of the control population ran from 2005 to 2009. Subsequently, the screening phase started in 2020 for the interventional cohort and 2012 for the control population. The screening phase will end in 2026 for the interventional cohort and 2024 for the observational cohort. These timelines are designed to ensure that all women who entered the screening programme at age 45 are screened until they turn 50.
Study hypothesisThe interventional cohort is stratified into five subgroups based on breast density and individual risk, each associated with an imaging protocol expected to have greater sensitivity than mammography in the control cohort. The two-year screening interval for the two low-risk interventional subgroups (with low and high density, respectively) compared with the control cohort (annual mammography) does not denote de-escalation, as digital breast tomosynthesis remains more sensitive than mammography. In brief, the study hypothesis predicts the superiority of the personalized screening approach in decreasing the cumulative incidence of advanced breast cancer compared with the conventional “one-size-fits-all” mammography screening procedure.
Outcome measuresThe primary and secondary outcome measures are listed in Table 1. The primary measure of the effectiveness of screening stratified by breast density and risk, compared with conventional annual mammography, will be the cumulative incidence of advanced breast cancer. In particular, the focus will be on stage II or higher cancer throughout the follow-up period. Most of the secondary outcome measures are part of the core indicators used in the annual national survey of regional mammography screening programmes in Italy. These indicators were defined by the Italian Group for Mammography Screening and the Italian National Centre for Screening Monitoring [48]. They constitute the benchmark for reporting outcomes of breast cancer screening programmes in Italy.
Table 1 Primary and secondary outcome measures in the RIBBS studyTable 2 provides an overview of the additional analyses planned as part of the RIBBS study.
Table 2 Additional analyses planned as part of the RIBBS studyInclusion criteriaThe criteria for inclusion into the interventional and observational cohorts are shown in Table 3.
Table 3 Inclusion criteria for the interventional and observational cohorts of the RIBBS studyExclusion criteriaThe exclusion criteria for both cohorts are shown in Table 4.
Table 4 Exclusion criteria for the interventional and observational cohorts of the RIBBS studyData collection and managementData collection and management will adhere to general Italian data protection regulations, ensuring maximum privacy and security of participants' information.
For the interventional cohort, a database dedicated to the RIBBS study was developed. This repository includes several tables containing essential information, such as mean VBD, calculated with the Volpara software, individual risk factors included in the IBIS software for lifetime risk assessment based on the Tyrer-Cuzick risk model, recall data derived from double readings, and details obtained from any required diagnostic procedure, including histologic data from biopsies. The raw data will be accessible for a variety of analyses or subanalyses.
As regards the observational control cohort, primary records will be obtained from the Emilia-Romagna Region mammography screening data warehouse. These data provide comprehensive information on invitations, mammograms, diagnostic procedures for abnormal screening outcomes, and benign or malignant lesions detected by screening. The case series is linked with the population-based regional breast cancer registry to obtain additional information.
To identify incident cases of breast cancer, all women in the interventional and observational control cohorts will be linked to the Veneto and Emilia-Romagna Cancer Registries, respectively. Automated case registration through the Veneto Cancer Registry has recently demonstrated a high level of consistency and reliability [49]. Previous studies have also validated the record-linkage protocols in both registries [38, 50]. Primary information available from both registries includes sociodemographic characteristics, primary cancer site, TNM tumour stage, histologic type, and vital status.
Sample sizeSample size calculations focused specifically on the primary outcome measure of the personalized screening procedure. This primary outcome measure revolves around assessing the reduction in the incidence of advanced breast cancer in the interventional cohort compared with the observational control cohort.
Considering the real-world context of the study and the constraints associated with enrolling participants in both cohorts, the sample size calculations encountered some limitations. The enrollment of patients in both cohorts was limited by factors such as available space and tight timelines due to the initial approval period granted by the Veneto Region. This consequently prevented expansion of the cohorts beyond the approved period.
Given the impossibility of accurately determining the sample size required to detect a specific effect on the primary outcome with the desired statistical power, our approach involved estimating the minimum detectable reduction in the incidence of advanced BCs using the sample size provided and ensuring a minimum power of 80%. The sample sizes available to conduct a one-sided test comparing the null hypothesis H0: rate ratio ≥ 1.000 and the alternative Ha: rate ratio < 1.000, using the W5 Variance Stabilized test statistic, were determined in 43,000 subjects in the observational control cohort and 10,269 subjects in the total interventional screening cohort, both over a 5-year exposure period. With these designated sample sizes, the study is able to achieve a power of 80.5% in detecting an event rate ratio under the alternative hipothesis (RRa) of 0.810. The event rate in the observational control cohort (λ1) is estimated to be 0.004017, based on the incidence rate of BC at baseline. Specifically, the significance level (alpha) used in the test is 0.050.
Statistical analysisRegarding the primary objective of the study, which focuses on evaluating the impact of the personalized screening model on the cumulative incidence of advanced breast cancer (stage II or higher), a series of analyses are planned. Person-years at risk and follow-up duration will be calculated for both cohorts, starting from the date of first screening and continuing until the date of censoring or the end of follow-up, whichever comes first. The follow-up duration will be truncated at the 75th percentile of available follow-up times, as determined by the criterion proposed by Puliti et al. [51].
Woman age will be calculated at the date of the first screening. Cumulative age-standardized advanced breast cancer incidence rates will be calculated for both cohorts and then compared using the incidence rate ratio (IRR) along with 95% confidence interval (95% CI). Estimation of IRRs will be obtained by multivariable Poisson regression analysis.
To address potential dissimilarities (if any) in the risk of breast cancer between the two cohorts, incidence rates from the pre-intervention period will be used. Adjusting the IRR of advanced breast cancer will involve multiplying the unadjusted IRRs by the observed/expected ratio within the observational control cohort. Calculation of 95% CIs will be performed by a bootstrap procedure.
Dissemination planThe results of the study will be widely disseminated through rigorous publications in reputable peer-reviewed journals. In addition, results will be communicated through presentations at regional, national, and international workshops and conferences. The dissemination strategy will primarily target clinicians, researchers and crucial stakeholders, including scientific societies and the Italian regional healthcare authorities. To ensure transparency and adherence to reporting standards, the study will adhere to the 'REporting of studies Conducted using Observational Routinely collected health Data' (RECORD) guidelines.
Comments (0)