
Remember me
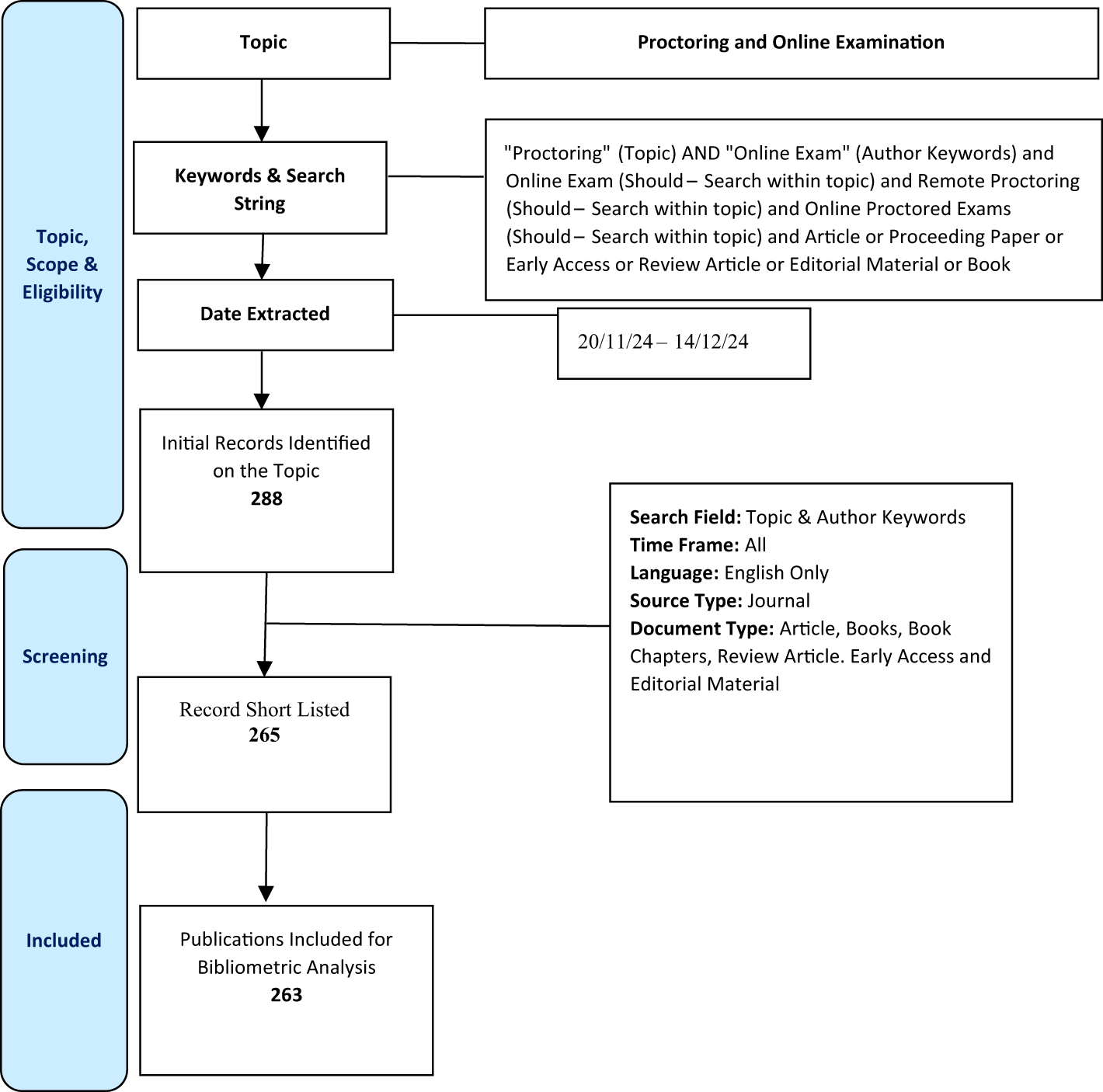

Consecutive patients who underwent clinically indicated contrast-enhanced CT of the abdomen were prospectively included in this study between December 2021 and June 2023. Inclusion criteria comprise the presence of a simple renal cystic lesion ≥ 10 mm in diameter and an available multiparametric MRI or ultrasound within reasonable temporal distance of the CT serving as reference standard. Patients were excluded if they had contraindications for contrast-enhanced CT imaging such as allergy to iodine contrast agent, renal impairment, and thyroid dysfunction, as well as individuals under 18 years of age. An overview of the study design is given in Fig. 1.
Fig. 1
Overview of the study design. All patients received clinically indicated multiphasic abdominal CT in PCD-CT. If a historical multiphasic abdominal CT on DE EID-CT was not already available, the clinically indicated follow-up examination was performed on DE EID-CT. aVNC = arterial virtual non-contrast; pvVNC = portal venous non-contrast; TNC = true non-contrast; PCD-CT = photon-counting detector CT; DE EID-CT = dual-energy integrating detector CT; MRI = Magnetic resonance imaging; US = Ultrasound
The local Institutional Review Board (Ethics Committee of the University Medical Center Freiburg, case number 21–2469) approved this prospective study and written informed consent was obtained from all patients before study inclusion.
CT imaging acquisition and reconstructionPCD-CT: All PCD-CT scans were obtained on a first-generation dual source PCD-CT scanner (NAEOTOM Alpha, Siemens Healthineers, Forchheim, Germany). The imaging protocol comprised a true non-contrast phase, an arterial phase, and a portal venous phase. First, the non-contrast scan was acquired followed by the arterial phase scan, which used contrast agent bolus tracking in the descending aortic for scan initiation after exceeding a threshold of 100 HU. For the portal venous scan, a fixed bolus delay of 80 s after contrast agent administration was used. Contrast agent (Iopromide, Ultravist 370 mg iodine/mL, Bayer Healthcare, Leverkusen, Germany) was administered using a dual-syringe power injector (Accutron CT-D Vision, Medtron, Saarbrücken, Germany) with a body weight adapted amount of contrast agent (1.2 mg/kg) followed by a 40 mL isotonic saline flush with a flow rate of 4.0 mL/s each. The acquisition parameters were as follows: tube voltage 120 kVp, automated attenuation-based tube current modulation with an image quality level (IQ Level) of 100 for non-contrast and arterial phase and 145 for the portal venous phase (99 effective mAs in non-contrast and 100 mAs in arterial and portal venous scans), pitch factor 0.8, collimation 144 × 0.40 mm, rotation time 0.5 s.
From the acquired spectral data of all scans, axial virtual monoenergetic images at 70 keV were calculated using a standard soft tissue kernel (Br40) with a slice thickness of 3.0 mm, an increment of 3 mm and Quantum Iterative Reconstruction (QIR) with strength 4. In addition, VNC images were calculated from the arterial and portal venous images using similar reconstruction parameters.
DE EID-CT: All DE EID-CT scans were acquired on a third-generation DE EID-CT scanner (SOMATOM Force, Siemens Healthineers, Forchheim, Germany). The institutional imaging protocol comprised true non-contrast scans, arterial phase scans (using bolus tracking with a threshold of 100 HU and a delay of 15 s) in single-energy mode and a portal venous scans in dual-energy (DE) mode 80 s after body weight adapted (1.2 mg/kg) contrast agent administration (Iopromide, Ultravist 370 mg iodine/mL, Bayer Healthcare, Leverkusen, Germany) using a dual-syringe power injector (Accutron CT-D Vision, Medtron, Saarbrücken, Germany) followed by a saline flush of 40 mL with a flow rate of 4 mL/s similar to the PCD-CT protocol. As the arterial phase scans were acquired in single-energy mode and no VNC reconstructions could be calculated, they were not included in any further analysis.
Acquisition parameters for the true non-contrast images were as follows: 100 kV, automated attenuation-based tube current modulation with a quality reference mAs of 147 mAs, rotation time 0.5 s, pitch factor 0.6, collimation 192 × 0.6 mm. For the portal venous phase reconstruction, the following parameters were used: DE mode with tube voltages of 90 kV and Sn150 kV, automated attenuation-based tube current modulation with quality reference mAs of 152 mAs and 95 mAs, rotation time 0.5 s, pitch factor 0.6, collimation 128 × 0.6 mm.
From the acquired raw data, we reconstructed axial series using a standard soft tissue kernel (Bf40) with 3.0 mm slice thickness and 3 mm increment and Advanced Modeled Iterative Reconstruction (ADMIRE) with strength 3.
In addition, VNC images were calculated from the portal venous series using the same reconstruction parameters.
Definition and reference imaging for verification of simple cystic lesions: Cystic renal lesions were defined following the Bosniak classification [7]. A simple renal cystic lesion eligible for inclusion in this study was defined as thin-walled (≤ 2 mm), well-defined, round/oval homogeneous fluid filled lesion with no septation, calcification or solid components and no enhancement (≤ 20 HU on CT).
In all patients, the presence of a simple renal cystic lesion was verified by additional renal imaging (ultrasound or MRI) serving as reference standard.
All ultrasound examinations were performed by board-certified specialists. Simple cystic lesions were defined as oval/round anechoic collections with a thin and smooth wall, no internal flow, no septations or solid components and presence of posterior acoustic enhancement.
MRI was performed as a multiparametric protocol comprising axial and coronal T2-weighted imaging, diffusion-weighted imaging and contrast-enhanced sequences on 1.5 T or 3 T scanners. Simple cystic lesions were diagnosed if the lesion showed high signal on T2-weighted images, no contrast enhancement or diffusion restriction and no septation or solid components. Simple cystic lesions with internal hemorrhage were defined if a lesion presented with high signal on unenhanced T1-weighted imaging, no contrast enhancement and no diffusion restriction. All MRI scans were interpreted by board-certified radiologists in a routine clinical reading session unrelated to the current study.
Image analysisIf a simple renal cystic lesion > 1 cm was present and verified by MRI or ultrasound, the value of VNC images was measured from arterial phase PCD-CT (aVNC PCD-CT), portal venous PCD-CT (pvVNC PCD-CT) and pv DE EID-CT (pvVNC DE EID-CT) images to compare the absolute density values and the enhancement in a two-step approach.
Density measurements of cystic lesions: In a first step, density measurements were performed in true non-contrast (PCD-CT and DE EID-CT) and VNC reconstructions (aVNC PCD-CT, pvVNC PCD-CT, pvVNC DE EID-CT) by placing identical regions of interest (ROIs) with a size of 100 mm2 in the same area of the cysts. Subsequently, the mean HU values and standard deviations (SD) were obtained from these measurements (example given in Fig. 2). All measurements were performed by the same radiologists (SR) with 4 years of experience in abdominal CT imaging.
Fig. 2
Example of Density-measurements in a simple renal cyst on EID DE-CT and PCD-CT images using true non-contrast, portal venous and virtual non-contrast derived images (from left to right). While true enhancement is < 20 HU, EID DE-CT VNC-derived values are remarkably low leading to false-positive enhancement > 20 HU. PCD-CT = photon-counting detector CT; DE EID-CT = dual-energy integrating detector CT
Enhancement of cystic lesions: Cystic lesions can still be classified as simple if they have a density ≥ 20 HU on non-contrast scans (most likely due to intralesional hemorrhage) but show no enhancement (defined as 20 HU) on contrast-enhanced scans. To account for this in a second step, the enhancement of the cystic lesions was assessed between the contrast-enhanced series (arterial and portal venous PCD-CT images and portal venous DE EID-CT images) and the true non-contrast images as well as between the contrast-enhanced series and the corresponding VNC reconstructions (aVNC PCD-CT, pvVNC PCD-CT, pvVNC DE EID-CT) using the following equation:
$$ } \left( }} \right) = } \left( }} \right) - } \left( \right) $$
(1)
Radiation doseRadiation doses of the PCD-CT and EID-CT examinations were assessed and compared via the volume CT dose index (CTDIvol [mGy]) in the non-contrast and portal venous series. The investigated protocols were optimized for abdominal/renal indication specific imaging in clinical routine and not with respect to radiation dose.
Statistical analysisAll statistical analyses were performed using R Foundation for Statistical Computing (Version 4.2.1, Vienna, Austria). Continuous variables are presented as mean ± SD or median and interquartile ranges (IQR) as appropriate. For categorical variables, frequencies and percentages are reported. Density measurements of the PCD-CT series (true non-contrast, aVNC, pvVNC) were compared via repeated measure ANOVA and post-hoc pairwise comparison using the Tukey method. For DE EID-CT density measurements (true non-contrast vs. pvVNC), paired sample t tests were conducted. To evaluate a potential cystic enhancement, the absolute difference between the true non-contrast and corresponding VNC reconstruction was calculated. p values were considered statistically significant if < 0.05.
Comments (0)