
Remember me
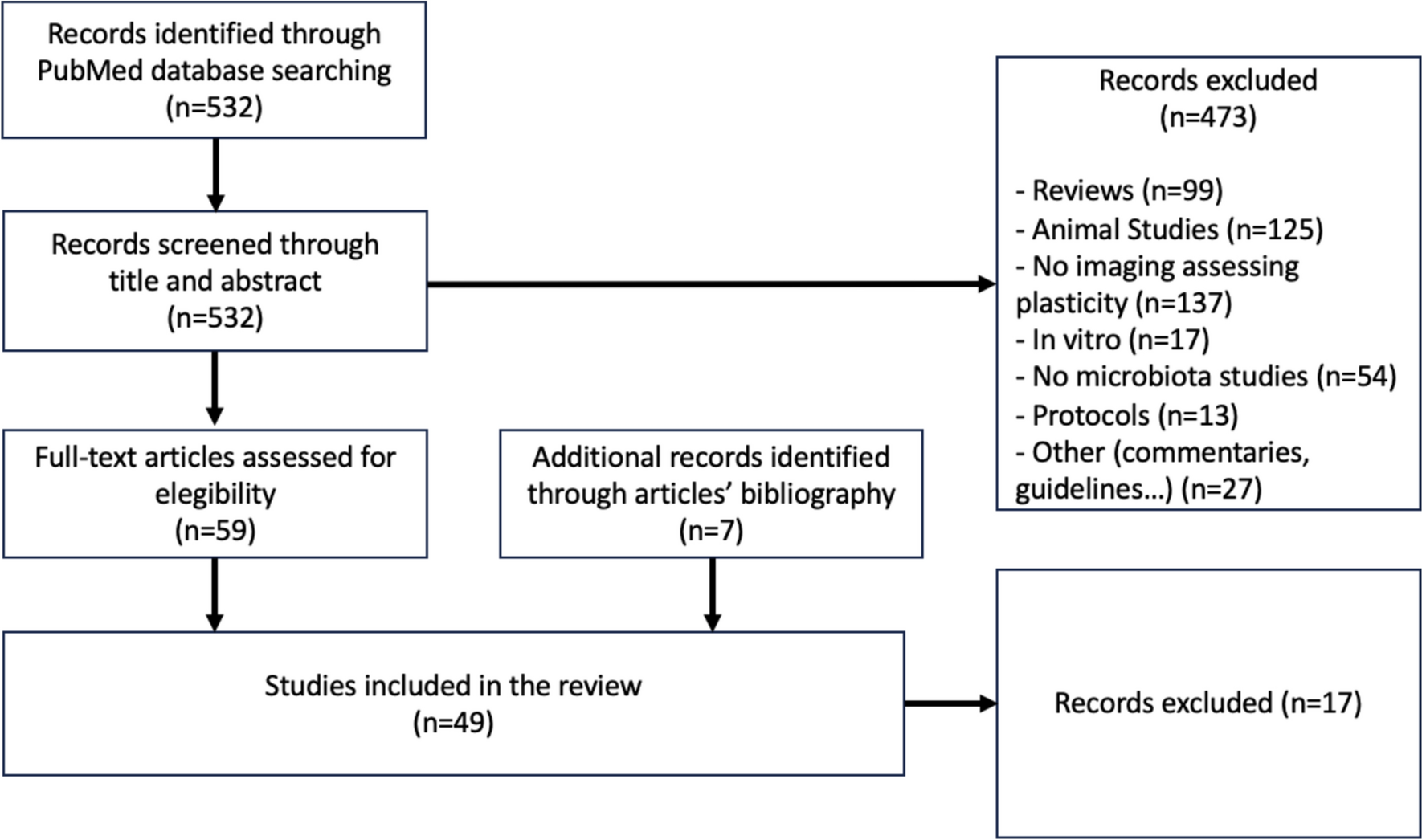
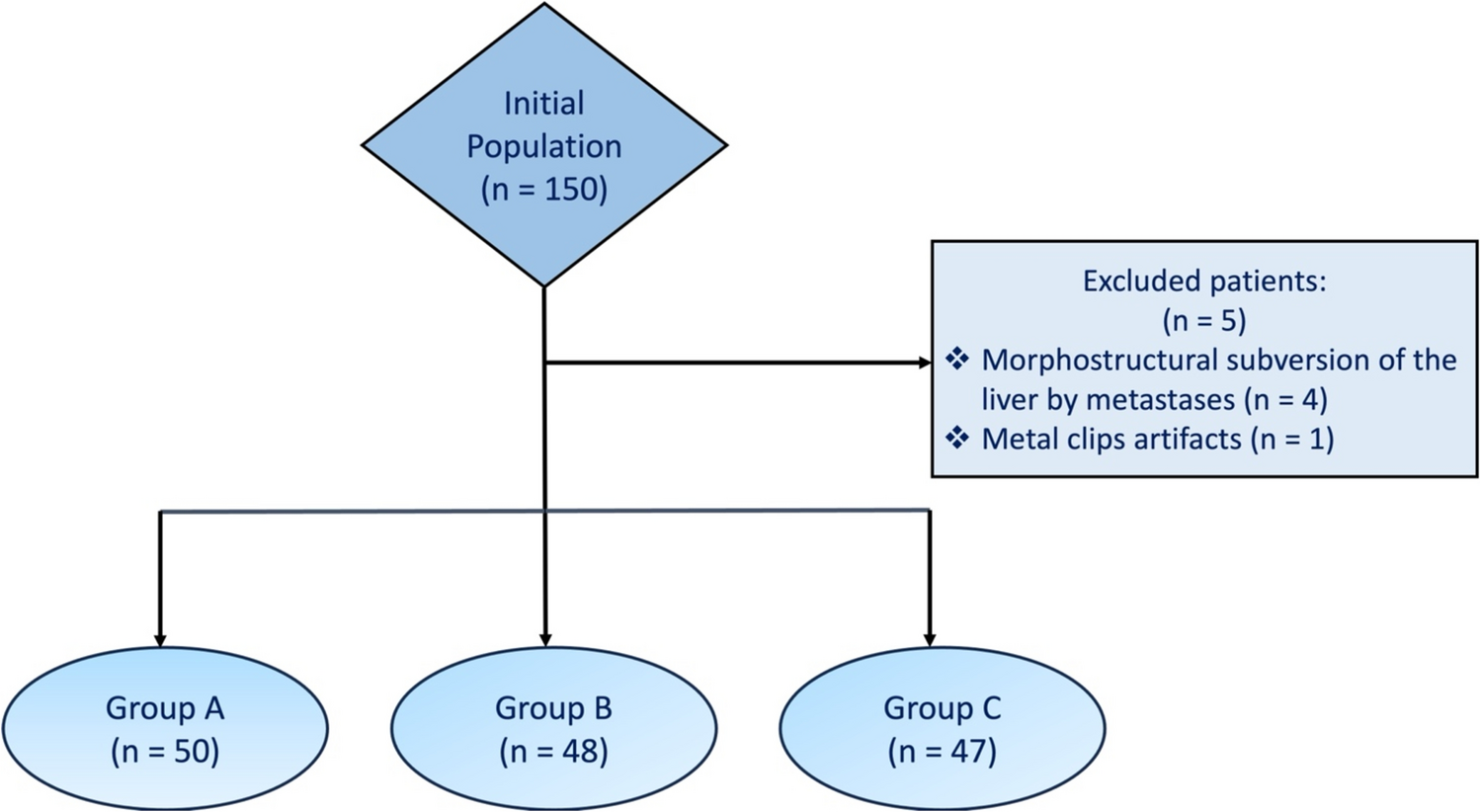




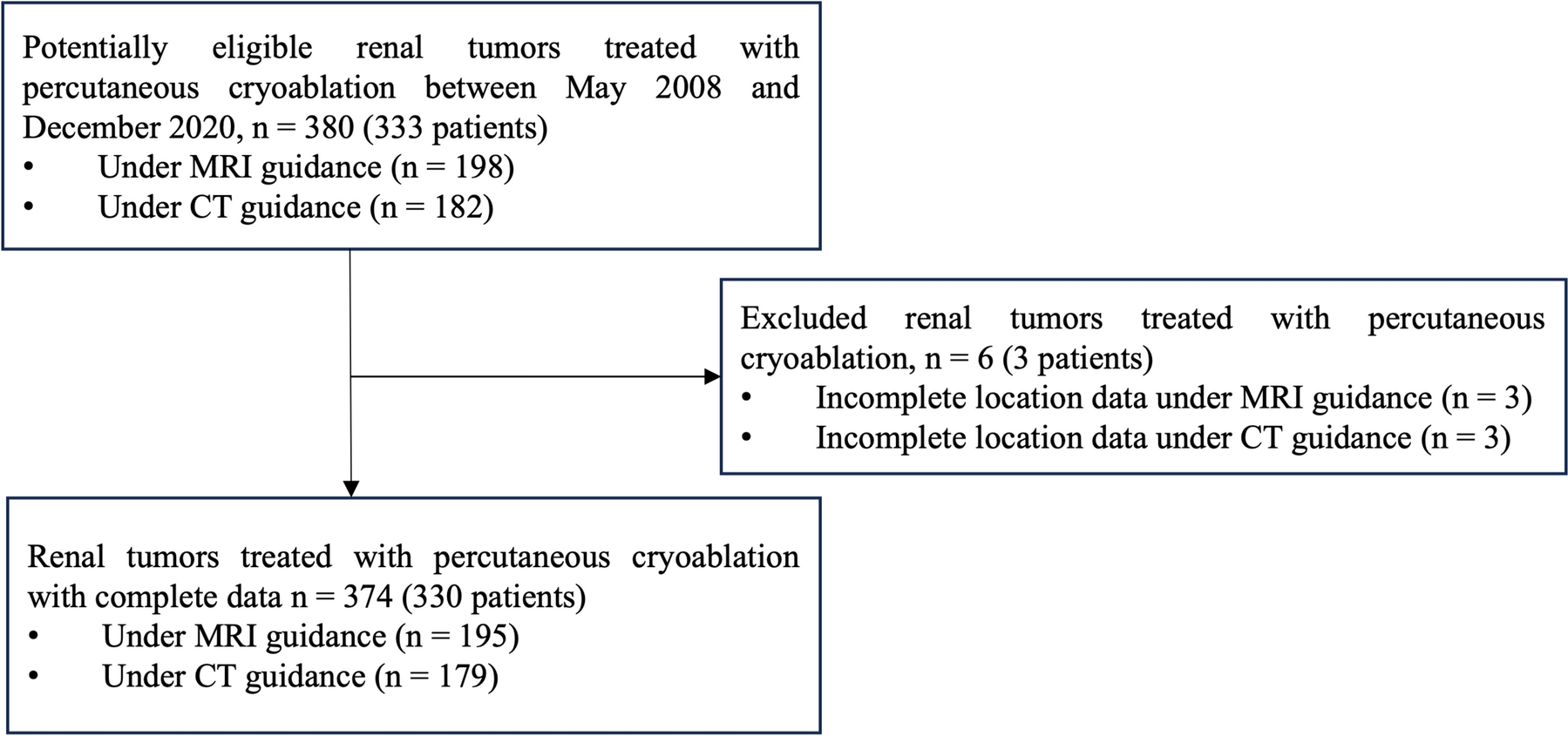
This retrospective study was approved by the institutional ethics committee of our institution (approval number: 2019-062), and informed consent for research participation was waived due to the retrospective nature. From June 2019 to October 2022, 1416 patients from two centers (center 1 = 907, center 2 = 509) were initially included according to the following inclusion criteria: (1) ILADC was surgically confirmed; (2) patients had undergone chest CT scans before operation; and (3) patients had not undergone any anti-tumor therapy before CT examination. Additionally, 446 patients were excluded according to the following exclusion criteria: (1) tumor confirmed with invasive mucinous adenocarcinoma, colloid adenocarcinoma, fetal adenocarcinoma, enteric type adenocarcinoma, or not otherwise specified (n = 41); (2) tumor manifested as synchronous multiple primary lung cancer (n = 327); (3) poor imaging quality due to obvious respiratory motion artifacts (n = 35); (4) ≥ 1-month interval between CT imaging and subsequent surgery (n = 43). Finally, the CT data of 970 patients (center 1 = 617, center 2 = 353) were used to build a DL model (model 1). Additionally, the CT data of 501 patients (center 1 = 208, center 2 = 293) with tumor diameters ≤ 2 cm were used to establish another DL model (model 2). Patients from center 1 were divided into the training and internal validation datasets in a ratio of 4:1, and those from center 2 were included as the external validation dataset. The patient inclusion flowchart is shown in Fig. 1.
Fig. 1
Patient inclusion flowchart
CT protocolsAll patients underwent chest CT scans using one of the following CT systems: Discovery 750 HD CT (GE Healthcare, Milwaukee, WI, USA), Somatom Perspective (GE Healthcare, Erlangen, Germany), or Somatom Definition FLASH (Siemens Healthcare, Forchheim, Germany). During a single breath-hold period, the CT scan was performed at the end of inspiration. The scan range was from the entrance of the thorax to the costophrenic angle. The scanning parameters were as follows: tube voltage, 100–130 kVp; automatic tube current, 50–250 mAs, scanning slice thickness/interval, 5 mm/5 mm, and reconstructed thickness/interval, 0.625–1 mm/0.625–1 mm. Then, all images were transferred to the picture archiving and communication system workstation.
Histochemical examinationHistological samples were obtained from surgical resection. All selected specimens stained with hematoxylin and eosin were analyzed by an experienced pathologist. According to the current LADC classification system, the percentage of some growth patterns (lepidic, acinar, papillary, micropapillary, solid) in the tumor with > 5% increments were considered to be indicative of this pattern.
Data preprocessingAll CT images in Digital Imaging and Communications in Medicine (DICOM) format were imported into the Infer Scholar Center platform (https://www.infervision.com/, Infer Scholar). Lesion region of interest (ROI) was initially manually denoted with bounding boxes slice by slice on axial CT images by a radiologist with 5 years of chest imaging experience, then that was reviewed and corrected by a radiologist with more than 10 years of chest imaging experience for accuracy. All the CT images were evaluated in a standard lung window setting to ensure optimal image quality and detail for accurate analysis. Thereafter, CT images were processed as follows: first, every 2D DICOM slice was concatenated to a 3D pixel matrix. Given that different image spacing will affect the recognition accuracy of 3D CNNs, the 3D pixel matrixes were resampled to obtain a 0.5 mm × 0.5 mm × 0.5 mm (height × width × depth) resolution with linear interpolation, and the pixel values were clipped to obtain lung windows (1400 HU, 200 HU). Second, all input images were normalized and padded to the same size. After acquiring these images, we randomly cropped them to 128 × 128 × 128 pixels and then performed random Gaussian noise, rotation, scaling, and flipping to reduce overfitting. Third, the augmented image patches were fed into the classification model for training. In the training process, to distinguish hard samples in the training set, we used self-paced learning (SPL), which can gradually incorporate hard samples into training. The initial threshold, threshold growth rate, and start epoch of SPL were 0.7, 1.05, and 20, respectively.
DL models establishment and optimizationTwo DL models were established in this study. Model 1 was used to predict the presence of M/S pattern in ILADC, and model 2 was used to predict the presence of M/S pattern in small-sized ILADC, which was defined as a tumor with a maximum diameter ≤ 2 cm in the lung window setting. Thereafter, 3D ResNet18 was adapted to build models, which included four-feature extraction stages and one classification stage. The number of output channels in the four-feature extraction stages were 64, 128, 256, and 512, respectively. The feature maps generated in the last feature-extraction stage were fed into the fully-connected layer to predict the probability of presence of M/S pattern. Adam W and cross entropy loss were used to optimize the classification models. The training batch size, learning rate, and epochs were 16, 0.0005, and 200, respectively. The workflow for model establishment, is shown in Fig. 2. The area under the curve (AUC), accuracy, recall, precision, and F1-score were used to evaluate the performance of both models. Additionally, another four DL networks, including ResNet34, ResNet50, ResNeXt50, and DenseNet121, were used to build models, and their performances were compared with those of 3D ResNet18.
Fig. 2
Workflow for model establishment
Statistical analysisTwo GTX 3090 graphics-processing units were used. The operating system was Ubuntu 20.04 with CUDA, version 11.3. Python 3.7 with PyTorch 1.11.0 were used to implement the models. Statistical analyses were performed with the SPSS 25.0 software package (version 25.0; IBM SPSS Statistics for Windows, IBM Corp., Armonk, NY, USA). The independent sample t-test was used to evaluate age, which was normally distributed, and P < 0.05 was considered to be indicative of a statistically significant difference.
Comments (0)