
Remember me
All procedures were performed in accordance with the protocol that was approved by the Research Ethics Committee of the Center for Data-driven Science and Artificial Intelligence, Tohoku University, Japan (registration number 2022–7). All subjects participated in this study gave their written informed consent.
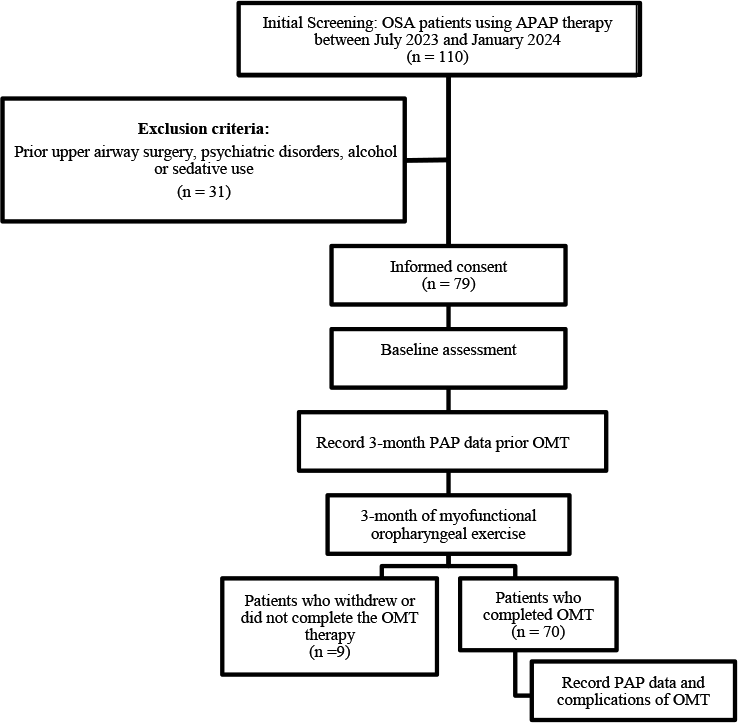
SubjectsThe eligible subjects for this study were patients who underwent an overnight polysomnography due to suspected or diagnosed sleep disordered breathing at Gifu Mates Sleep Clinic in Gifu, Japan, between September 2022 and December 2022. The inclusion criterion was adulthood (age 20 years or older). Subjects were excluded if they had continuous atrial fibrillation, experienced acute illness, or had exacerbation of chronic diseases requiring hospitalization within the past three months. Additionally, individuals who were pregnant or breastfeeding were also excluded.
ProtocolThe polysomnographic examination was performed with an Alice diagnostic sleep system (Philips-Respironics, Murrysville, PA, USA Philips Respironics, The Netherlands). The examination was initiated at the subject's customary bedtime and continued until the subject awoke the next morning, during which micromotions were continuously measured by a commercially available piezoelectric rubber sheet sensor device (Moni Life wellness®, Sumitomo Riko Company Limited, Komaki, Aichi, Japan).
Subjects were randomly allocated into a training group and a test group. Using the data from the training group, we developed and optimized the algorithms for sleep apnea detection, constructed regression models to estimate sleep apnea severity, and identified the optimal cutoff values for classifying the severity. Using the data from the test group, we evaluated the classification performance of the algorithms.
MeasurementsThe polysomnograms were recorded with the standard montages consisting of F4-M1, F4-M2, C4-M1, C3-M2, O2-M1, and O1-M2 electroencephalograms, left and right electrooculograms, a submental electromyogram, a nasal pressure cannula, oronasal airflows, left and right tibial electromyograms, thoracoabdominal inductance plethysmograms, pulse oximetric arterial blood oxygen saturation, a neck microphone, body position sensors, and a modified lead II ECG.
Sleep stages, apneic and hypopneic indices (AI and HI, respectively), and AHI were scored according to the American Association of Sleep Medicine (AASM) Manual for the Scoring of Sleep and Associated Events, Version 2.5 [19] by registered polysomnogram technicians. AHI was calculated both with the total recording time (TRT) as the denominator (AHITRT) and total sleep time (TST) as the denominator (AHITST). The AHITRT was used as the reference standard for developing algorithms for sleep apnea detection from the micromotion signal. The AHITST was used to classify sleep apnea severity, with < 5 defined as normal, 5–15 as mild, 15–30 as moderate, and ≥ 30 as severe sleep apnea. The ECG signal of the polygraph was sampled at a frequency of 100 Hz. All QRS complexes were identified and annotated as normal (sinus rhythm), ventricular ectopic beat, supraventricular ectopic beat, and artifact.
The piezoelectric rubber sheet sensor, depicted in Fig. 1, had dimensions of 811 mm in length, 60 mm in width, and 0.9 mm in thickness and a weight of 220 g. It was positioned beneath the bedsheet at a level from the subject's axilla to the lower end of the sternum body. The signal was digitized at 100 Hz with a 24-bit dynamic range (± 223, from -8,388,608 to + 8,388,608) and the device outputted the data to a CSV file.
Fig. 1
Schema of piezoelectric rubber sheet sensor used for measuring micromotion
Development of REI algorithmsThe details of the algorithms are reported in Appendix. Briefly, first, the algorithm extracted respiratory, body movement, and ballistocardiogram components from the micromotion signal of the piezoelectric rubber sheet sensor using band-pass filters set to their respective frequency ranges (0.08–0.5, 2–3, and 4–11 Hz) (Fig. 2). Second, the respiratory component signals were rectified to reflect the magnitude of respiratory motion and natural logarithm transformation was performed to minimize the effects of large changes in respiratory amplitude and large noise. Third, two types of upper (95th percentile point) envelopes (fast and slow) were generated; the fast envelope depicted breath-by-breath amplitude changes, while the slow envelope presented the local trend of submaximum amplitude. The use of the 95th percentile points for the envelopes excluded outliers with an incidence < 5%. Fourth, periods in which the fast envelope separated downward from the slow envelope to an extent greater than a threshold (depth threshold) were detected. Fifth, when the length of a period was within a range (duration criteria), the period was considered to be a respiratory event. Finally, REI was calculated as the frequency of respiratory events per hour of TRT.
Fig. 2
Detection of sleep apnea by micromotion signal from piezoelectric rubber sheet sensor. A series of sleep apnea attacks began to appear at 04:28, with the fast upper envelope of respiration (red line in panel b) declining from the slow upper envelope (blue line in panel b) and showing periodic dips. Panel d is the enlarged image of frame b’ in panel b. Periods in which the dip of the fast upper envelope (red line) from the slow upper envelope (blue line) exceeds a depth threshold (ln (1.43), which corresponds to a 30% drop) are indicated by vertical lines (cyan). When the length (L) of a period meets duration criteria (10 to 70 s), the period is considered to be a respiratory event
The optimal values of depth threshold and duration criteria were determined in the training group using a grid-search method. This involved repeated analyses with small parameter adjustments until the closest correlation between REI and AHI was achieved. Because the amplitude of respiratory movement detected by the sheet sensor varied substantially with body position, a percentage reduction was employed as the depth threshold to adapt to the variations. The search for the optimal depth threshold was conducted in 1% increments, while the optimal lower and upper duration criteria were determined at 10-s intervals.
The source code for these algorithms was written in FORTRAN 95 and compiled on Microsoft Windows 10 by the Silverfrost Fortran (FTN95) compiler (Elgin, IL, USA).
Analysis of FcvFcv was measured not only from the heartbeat interval of the ballistocardiogram but also from ECG R-R interval of the polysomnography (ECG-Fcv). The method for measuring the heartbeat interval from ballistocardiogram is reported in Appendix. CVHR was detected by previously published algorithm [7, 8, 18] and Fcv and ECG-Fcv was computed as the frequency of CVHR per hour of TRT. The ECG-Fcv was used to determine whether the association between ballistocardiogram Fcv and AHITRT is affected by the accuracy of ballistocardiogram-based heartbeat interval measurement.
Statistical analysisThe statistical analyses were performed using the program package of Statistical Analysis System (SAS Institute, Cary, NC, USA). Between-group differences in quantitative and categorical variables were assessed using the Wilcoxon rank sum test and χ2 test, respectively. The relationships between AHITRT and REI, Fcv, and ECG-Fcv were evaluated with Pearson's correlation coefficient. The multivariate regressions were performed using the SAS REG procedure. The classification performance of REI, Fcv, and ECG-Fcv for binary sleep apnea severity was evaluated by the area under the curve (AUC) of the receiver-operating characteristic (ROC) curve. The classification performance for four severity levels (normal, mild, moderate, and severe) was examined by the percentages of subjects correctly classified and misclassified off by one, two, and three classes. The optimal REI cutoff values for these classifications were determined by balancing sensitivity and specificity by ROC curve analysis in the training group and then evaluated in the test group. Statistical significance was defined as P < 0.05.
Comments (0)