
Remember me

This study utilised routine electronic health records from the clinical management system under the Hospital Authority (HA) of HK and vaccination records from the Department of Health (DH) of the HK Government. These two databases are linked using the unique HK Identity Card Number or other personal identification numbers. The HA is a statutory administrative organisation in HK that manages all public inpatient and outpatient services. The clinical management system, which includes demographics, diagnoses, prescriptions, and laboratory tests, provides real-time data support and monitoring for routine clinical management across all clinics and hospitals in HA. On the other hand, the DH manages and retains the database for all vaccination records in HK. The two population-based databases have been used previously to conduct studies on the risk of adverse effects after COVID-19 vaccinations and other COVID-19 pharmacovigilance studies [16,17,18].
2.2 Study PopulationThe study population included those aged ≥ 18 years who had either been hospitalised for COPD or asthma before the start of the study (specifics outlined in each study design). The International Classification of Disease Ninth version, Clinical Modification (ICD-9-CM) codes, and British National Formula (BNF) codes are shown in Supplementary Table 1. Our primary analysis included people with COPD or asthma, or both, as some may have both conditions concurrently. Subgroup analysis was conducted to differentiate between admissions related to COPD and asthma.
2.3 A Self-Controlled Case Series (SCCS) for Severe ExacerbationThe SCCS design was applied to investigate the risk of severe respiratory exacerbation following administration of CoronaVac or BNT162b2 between 23 February 2021 and 30 November 2022 (observational period). The SCCS is a within-individual study design that compares the incidence of outcomes during the exposure period to the non-exposure period within the same individual. Therefore, it inherently controls for known and unmeasured time-invariant confounders. Additionally, time-varying confounders such as seasonality effects can be adjusted for within the regression model.
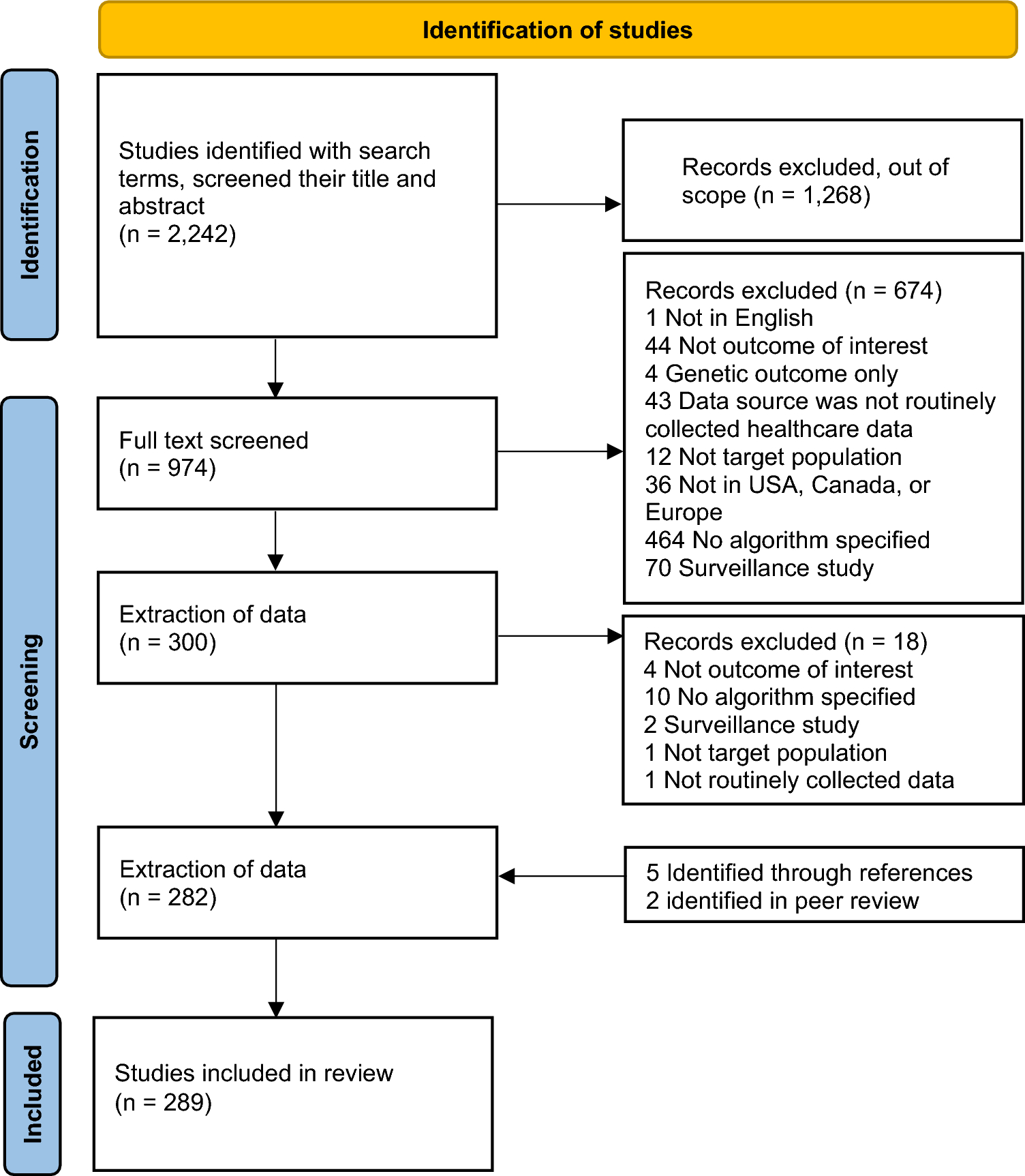
We identified people with COPD and asthma who had exacerbation during the observational period for the SCCS. The flowchart outlining the selection process for the SCCS population is shown in Fig. 1. The primary outcome of interest for the SCCS was severe respiratory exacerbation, defined as the first hospitalisation for asthma or COPD or respiratory failure of any cause. The exacerbations were determined according to published case reports [8,9,10,11]. Patients who received heterologous COVID-19 vaccines or were diagnosed with COVID-19 infection before 30 November 2022 were excluded from the analysis since the COVID-19 infection may increase exacerbations that would bias the results.
Fig. 1
Flowchart of cohort selection for SCCS (vaccine safety) and cohort study (vaccine effectiveness) for two doses of COVID-19 vaccines. COPD chronic obstructive pulmonary disease, COVID coronavirus disease, HA Hospital Authority, N number, SCCS self-controlled case series
Since respiratory exacerbation after vaccination could potentially impact subsequent exposure, we applied a modified SCCS extension developed for event-dependent exposure [19]. The modified SCCS model incorporated unvaccinated patients who experienced outcome events during the observational periods to account for the probability of receiving vaccination after the event. Including unvaccinated patients was a control to provide a baseline comparison for the vaccinated group.
The risk periods were defined as 28 days after administering the first, second, third, and fourth doses. Based on case reports showing that the acute respiratory events occurred within 7 days after vaccination, we further divided the risk periods into 0–7 days and 8–28 days after each dose. The rest of the study period was defined as the baseline period. A schematic presentation of the SCCS design is shown in Fig. 2. Since no trial was conducted to examine the risk of respiratory exacerbation after COVID-19 vaccination, a relative risk of 1.1–3.0 was assumed based on our team’s previous COVID-19 vaccine safety studies [20,21,22]. This corresponded to a required sample size of 70–6430 events to achieve 80% power at a significance level of 0.05 for the SCCS analysis, considering an observation period of 650 days.
Fig. 2
Self-controlled case series (SCCS) study design
2.4 Retrospective Cohort Study for Vaccine EffectivenessWe identified patients with COPD and asthma (study population) before 23 February 2021. Vaccinated patients were those who had received two homogenous doses of COVID-19 vaccines. The index date for vaccinated patients was defined as the date of their second dose. People who had received heterogeneous first two doses before 30 November 2022 were excluded from the analysis. Before 30 November 2022, patients who did not receive COVID-19 vaccines were considered unvaccinated. For each vaccinated patient, a randomly selected unvaccinated patient of the same age and sex was matched, and the second dose vaccination date from the vaccinated patient was assigned as the pseudo-index date for the matched unvaccinated individual. Patients in the control group who died before the pseudo-index date were excluded from the analysis.
People were followed up from the index date (pseudo-index date for unvaccinated individuals) until the end of the study (30 November 2022), the occurrence of the outcome, the date of the next vaccine dose, or the date of death, whichever came first. For the analysis of VE regarding the fourth dose, the cohort was followed up until the end of the study, the occurrence of the outcome or date of death, whichever came first. The schematic presentation of the cohort study is shown in Supplementary Figure 1.
The primary outcomes were defined as COVID-related mortality and hospitalisation. COVID-related mortality was defined as non-injury or poisoning-related mortality within 28 days after a positive polymerase chain reaction (PCR) test for COVID-19. This definition aligns with the guidelines and recommendations provided by the World Health Organisation [23]. COVID-related hospitalisation was defined as all-cause hospitalisation within 28 days after a positive PCR test for COVID-19. The rationale for choosing this co-primary outcome was that it provides important information about disease severity and its impact on people’s health. In addition, this result may provide evidence to guide policy decisions and resource needs in future pandemics. The secondary outcome was COVID-related severe complications, defined as admission to the intensive care unit or use of ventilatory support within 14 days after a positive PCR test for COVID-19 [24].
We identified the baseline characteristics, including sex and age, at the index date. Comorbidities and Charlson score were identified using a 3-year lookback period before 23 February 2021. Prior medications were identified within a 1-year lookback period before 23 February 2021. The comorbidities and previous medications are shown in Table 1.
Table 1 Baseline characteristics for the study cohort, separated by unvaccinated, two doses of CoronaVac and BNT162b22.5 Statistical AnalysisThe safety study estimated the incidence of outcomes following COVID-19 vaccines, reported as cases per 100,000 doses. The analysis utilised a conditional Poisson regression model to estimate the incidence rate ratio (IRR) and its corresponding 95% confidence interval (CI). This involved comparing the incidence rates of respiratory exacerbation during different risk periods to the baseline period while adjusting for the monthly seasonality effect.
For the effectiveness study, a propensity score-based inverse-probability-of-treatment weighted Cox proportional hazard model was used to estimate the weighted hazard ratio (HR) of COVID-related outcomes. This analysis compared people who received two, three, and four vaccine doses to those who were unvaccinated. The VE was evaluated by (1 − adjusted HR) × 100%. The propensity score was calculated using multinomial logistic regression models, including all covariates as potential predictors for the COVID-19 vaccinated group. Extreme weight values were truncated at the 5th and 95th percentile of the distribution to mitigate the influence of outliers.
2.6 Subgroup AnalysisSeveral subgroup analyses were conducted to examine the robustness of the primary analysis results. Stratification was carried out based on people with admission for COPD or asthma, sex, and age group (< 65 years and ≥ 65 years) for subgroup analysis in both exacerbations and effectiveness studies. A subgroup analysis was also conducted on patients who had previously experienced respiratory failure (before 23 February 2021), as they may be at a higher risk of severe outcomes following COVID-19 infection. However, subgroup analyses were not performed for people who received the third and fourth vaccine doses due to the limited sample size available for analysis.
All statistical tests were two-sided, and p values < 0.05 were considered significant. Statistical analyses were conducted using R version 4.1.2 and SAS version 9.4 (SAS Institute, Inc, Cary, NC). To ensure quality assurance, two authors (co-first authors) independently performed the statistical analyses. The transparent reporting of this cohort study followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement checklists to enhance the clarity and completeness of the study report.
Comments (0)