
Remember me
In total, 12 participants were recruited and interviewed for this study (Table 1). All participants were pharmacy undergraduate students studying at one School of Pharmacy in the UK. Eight interviews were conducted as individuals and two interviews were conducted in pairs. Considering their pharmacy education level, one participant was in their first year of study (9%), four were in their second year (33%), four were in their third year (33%) and three were in their fourth year (25%). Participant self-reported ethnicities included a range of minority and majority groups, and included the views of five international students. There were no refusals to partake, participant drop outs or repeat interviews.
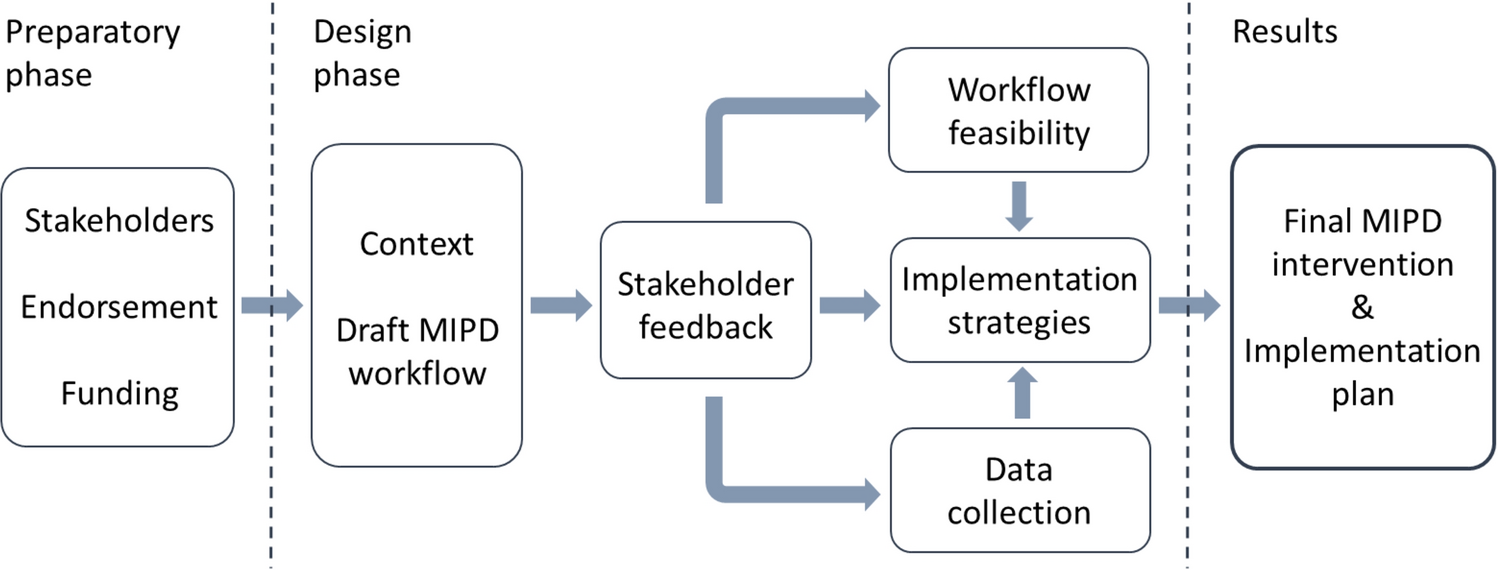
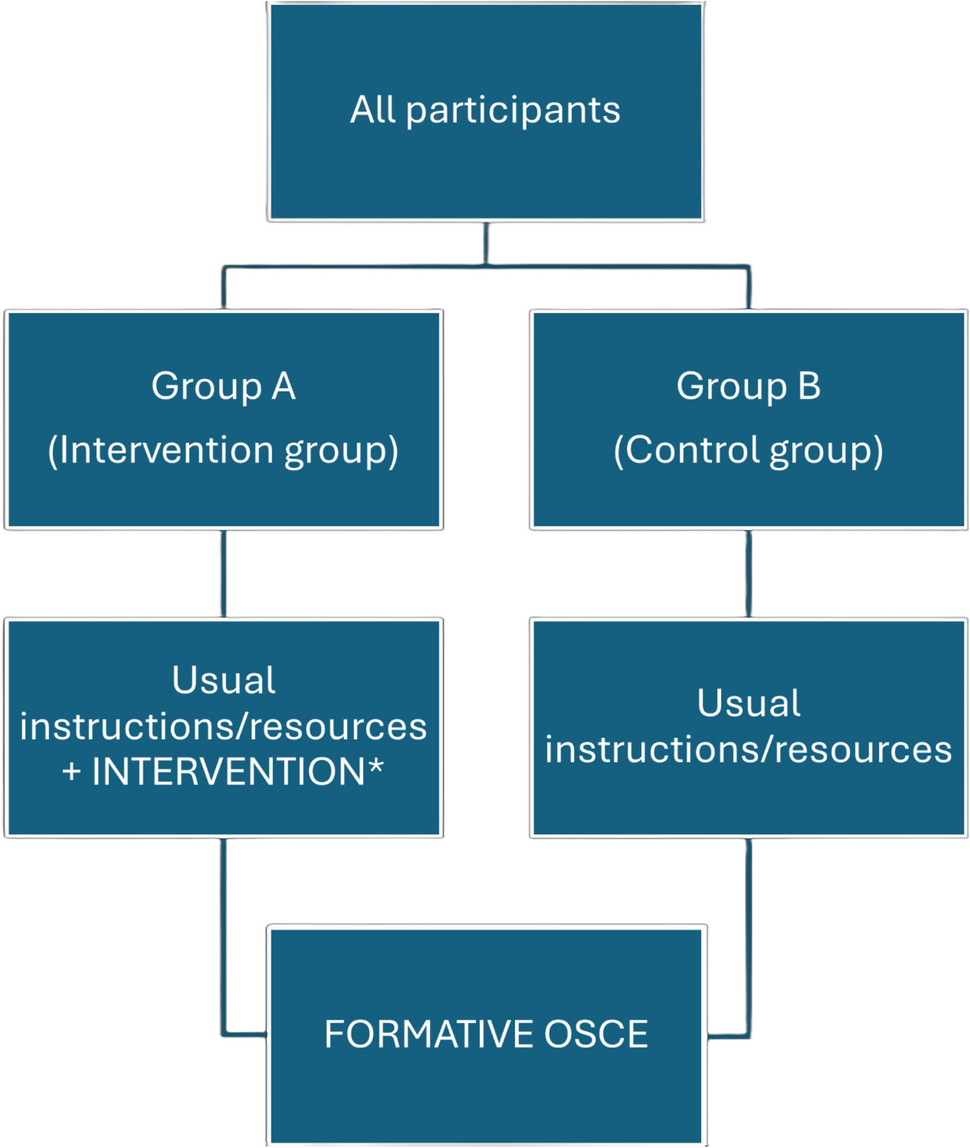
Three overarching themes were developed to reflect the perceptions of pharmacy students on the integration of cultural competency and cultural humility within pharmacy education: (1) recognising and reflecting on cultural competency and cultural humility; (2) gaining exposure and growing in confidence with cultural competency training; and (3) thinking forward as a culturally competent pharmacist of the future (Fig. 1). The three themes, and their sub-themes, are discussed in turn (Table 2 contains further quotes).
Fig. 1
The three themes and sub-themes developed in this study which appear fundamental in shaping the initial education and training of pharmacy students underpinned by cultural competency and cultural humility. The double-ended arrow and choice of colours indicate the iterative personal development and education in the space of cultural competency –the red colour represents processes of recognition and self-reflection; the amber colour indicates strategies to promote growth in confidence; and green denotes the forward thinking approaches of a culturally competent pharmacist when practicing in the future
Table 2 Additional verbatim quotes included to illustrate the themes and sub-themes of this workTheme 1: Recognising and reflecting on cultural competency and cultural humilityWithin ourselves and in our student cohortMany participants began by reflecting on what they knew and understood cultural competency to be. Two students described understanding cultural competency as being centred in awareness. One student in their second year of pharmacy education described
“being culturally competent… I feel like it’s mostly just being aware of like, differences, across different people and cultures” (Participant 2, Stage 2).
One student shared how their upbringing has shaped their appreciation for diversity within people and places, describing
“where I lived growing up, it was in a really multi-cultural place with people of all ethnicities in my school, class, friendship groups… that’s just normal to me – to me, cultural competency is probably viewing society and others in a non-judgemental way… but maybe that’s not the same for everyone” (Participant 1, Stage 1).
Another student reflected only becoming aware of wider diversity and cultures
“only really when I moved to University and began to mix with more wider diverse people and started learning more about other ways of doing things” (Participant 2, Stage 2).
“I can see why it (cultural competency) is important because it’s encouraging you to open your eyes and mind more and if we’re going to be pharmacists, we need to show we care about other people’s beliefs” (Participant 2, Stage 2).
Within our patientsStudents also demonstrated reflections that extended beyond themselves, to the patient population they would be providing care for. One final year student described culturally competent approaches as those which identify each patient as
“unique and treating them as such”, instead of adopting a style of “a one-size-fits-all” (Participant 6, Stage 4).
Many students noted that cultural competency and cultural humility extended beyond ethnicity as a single entity. Instead, students discussed considerations that take
“into account people’s culture—there’s aspects of religion, race, ethnicity, sexual orientation, the list can go on… it’s important you factor in the whole person” (Participant 5, Stage 4).
Students illuded to the importance of learning about wider issues that may also impact a person in receipt of healthcare, such as their sexual orientation.
“As much as it (cultural competency training) should be learning about like race and ethnicity factors, we cannot forget about learning about other factors that like, make up a person, like if they are gay or transgender that we’re treating” (Participant 3, Stage 3).
Two students made the connection between cultural competency and the General Pharmaceutical Council (GPhC) standards for pharmacy professionals, particularly in relation to person-centred care. One student stated
“cultural competency – it’s important for us to learn about because it also adheres to the GPhC’s standards, like we’re actually showing that we care about the person’s beliefs and they don’t feel just like a case to be solved” (Participant 12, Stage 2).
Theme 2: Gaining exposure and growing in confidence with cultural competency trainingWhen is the best time to teach cultural competency?One of the main points of discussion in interviews was the need to grow student confidence, specifically by gaining exposure to issues exploring cultural competency within their education. Students suggested a number of ways of when cultural competency and cultural humility should feature within their training to gain this required exposure. One such suggestion centred around taught materials “like specific seminar classes” which were aimed at
“introducing the concept at the very start (of the undergraduate degree) so you’re made aware of what it is at a basic level” (Participant 3, Stage 3).
“When you start learning more clinical things, like from stage 2 onwards, and when it gets more complicated in stage 3 and 4, you need to be bringing the cultural focus back to everything – so if you’ve already covered it from stage 1, then it should become second nature” (Participant 5, Stage 4).
All student participants commented that the teaching of cultural competency should continue throughout the degree. But rather than taking place in standalone session(s), students felt that content should be embedded throughout all aspects of the degree. One student described
“rather than it being titled ‘this is your cultural competency teaching’ … I think it would be actually better if it featured a little bit in everything we do” (Participant 11, Stage 4).
Another student recognised the reality of the diverse people they will be treating once qualified, citing this as the reason to weave cultural competency education throughout (Table 2).
How should cultural competency be taught?Recommendations were also made around the approaches and teaching styles that may be best suited for embedding cultural competency training within the current curriculum. Many participants drew connections between the learning environments that may be better suited for embedding cultural competency training within the current curriculum. Seminar classes, or classes that were smaller in size and more interactive than lectures, were deemed an ideal environment for cultural competency to be visited, and re-visited. Teaching that was linked to a patient case and where it echoed a real-life scenario was viewed as the most desirable (Table 2).
There was a connection linking cultural competency education with supporting the knowledge, as well as confidence, of pharmacy students. One second year student spoke of wanting
“to feel more confident in the language I use or terms I use when I’m talking about this (cultural competency) so, to be honest, I would prefer it (teaching) to be in a smaller group so I’m not… embarrassed if I got it wrong” (Participant 2, Stage 2).
A first year student indicated their readiness to learn, but also the need for confidence, as they discussed wanting
“to just be able to learn, and have the knowledge, and have the confidence really to conduct a review with anyone, any type of person” (Participant 1, Stage 1).
A final year student reflected upon the development in their confidence and communication over time, recognising
“I was not confident about what words to even use at the start, but now, like there’s definitely been progress and I do feel more confident in thinking that way (with cultural competency)” (Participant 11, Stage 4).
It appeared that laying the foundations at the start of the degree, and building upon them throughout their education, was a desirable approach to take.
Other examples of opportunities to learn and develop cultural competency skills included experiential learning, specifically on placement. Many students, across all years of study, described the patient contact time they experienced on multi-sector pharmacy placements (a standard learning experience within their degree) as a key opportunity to put their learning into practice. Students discussed the value and benefit of hearing first-hand the lived-experiences of
“the actual people experiencing this… they should be the ones feeding back and keeping us right (around issues relating to cultural competency) as they’re living it” (Participant 5, Stage 4).
Theme 3: Thinking forward as a culturally competent pharmacist-of-the-futureCultural competency underpinning clinical decision makingThinking forward on their educational trajectory to becoming pharmacists, students acknowledged and shared examples of where cultural competency training can support them in clinical decision-making alongside patients. Students across stages two, three and four appreciated the importance of tailoring care to an individuals’ needs but they also extended this to encompass culture in the examples they provided. Many of these examples related to supporting the safe and effective use of medicines and, in particular, involved a patient from a minoritised community (see Table 2).
“Doing something in reality that I’d learnt about in the classroom ... a man of South Asian descent came to me on placement asking me about his medicines, well, the fact he wants to miss taking his medicines when it’s Ramadan ... I was able to help him because of what we’d covered in seminars” (Participant 11, Stage 4).
Second year students also eluded to the importance of appreciating person-centred ethnic considerations when diagnosing and treating disease; they discussed
“in hypertension, there’s certain ethnic groups that you can’t give ACE-inhibitors to … that’s really important for us to know to make sure we’re keeping patients safe” (Participant 7, Stage 3).
Another indicated the importance of including diversity within teaching materials, given that some dermatology conditions have
“some physical signs that you can see, but on certain skin colours, you can’t see the effects or it might look totally different” (Participant 8, Stage 2).
Students also acknowledged that cultural competency teaching can extend beyond the discipline of pharmacy practice. One student described how culturally competent approaches in the specialty of pharmaceutics has supported their knowledge of excipient suitability, given that
“certain religions can’t have certain ingredients, meaning certain medications are unsuitable … like those that have meat products in, or alcohol content” (Participant 8, Stage 2).
Continual learning and development to be culturally competentStudents also acknowledged that there is, and will always be, need for them to practice ongoing, continual personal development. When considering their education and training, students were mindful of the fast-paced changes and updates relating to cultural competency; one student discussed
“the terminology is changing all of the time, now even ‘BAME’, as a term, that was used loads fairly recently but even now it’s fading” (Participant 1, Stage 1).
“(Being a culturally competent pharmacist), it’s definitely going to be an ongoing process, we can’t know everything, but we can try to learn as much as possible because all patients need us to approach them sensitively” (Participant 11, Stage 4).
Developing cultural competency skills outside of the profession and transferring them into their role as a future pharmacist was also discussed. Students discussed
“independent learning that I could do myself, like reading up on the news and social media about how people are speaking up for trans rights… that can all feed back into my job and patients I’m seeing” (Participant 3, Stage 3).
Many students described reflective approaches that could be integrated into their personal and professional development. One student considered how
“writing reflective pieces on being in the scenario where cultural competency is required… it should be done as reflecting improves who you are as a pharmacist” (Participant 8, Stage 2).
A final year student considered ways that their pharmacy postgraduate education could continue the links established at an undergraduate level, including focus on cultural competency (Table 2).
Comments (0)