
Remember me









Heartburn and regurgitation are common symptoms, experienced regularly by up to 20–50% of individuals [1,2]. Individuals with mild heartburn frequently use over-the-counter antacids, while those with more severe symptoms often resort to long-term use of acid-suppressant medications. This acid-centred approach, which is highly effective for healing reflux oesophagitis, ignores the more complex aetiology of oesophageal symptoms, wherein dietary habits, reflux hypersensitivity, psychosocial factors and obesity, may also play a role [3–5]. However, the impracticality of exploring this complex symptom aetiology compared with the pragmatic approach of using proton pump inhibitors (PPIs) has led to widespread, open-ended PPI use. Unfortunately, this also means that reflux-like symptoms, the severity of which exhibits only a weak relationship with pathological oesophageal acid exposure, continue to impact the day-to-day lives of a large proportion of individuals [1,6].
The concept that dietary and lifestyle factors can influence the likelihood of reflux-like symptoms is well accepted. However, patients are generally given minimal (and inconsistent) advice about implementing diet, lifestyle and behavioural changes [7–10], despite these being low-harm, pragmatic approaches to self-management. One reason for this is a historical lack of emphasis in evidence-based clinical guidelines, which stems from a paucity of high-quality interventional studies. Ideally, guidelines and clinical advice should be based on rigorous evidence, for which randomised controlled trials (RCTs) are the gold standard. However, a lack of RCT evidence does not negate the value of ‘lifestyle’ recommendations. Hence, the Delphi method, with greater emphasis on clinical experience and expert consensus, was used to develop a set of consensus statements of advice to help providers and patients target the physical and perceptual factors contributing to reflux-like symptoms. These statements can serve as a basis for facilitating doctor-patient communication as well as aiding the development of self-management tools to better support the wellbeing of patients with reflux-like symptoms.
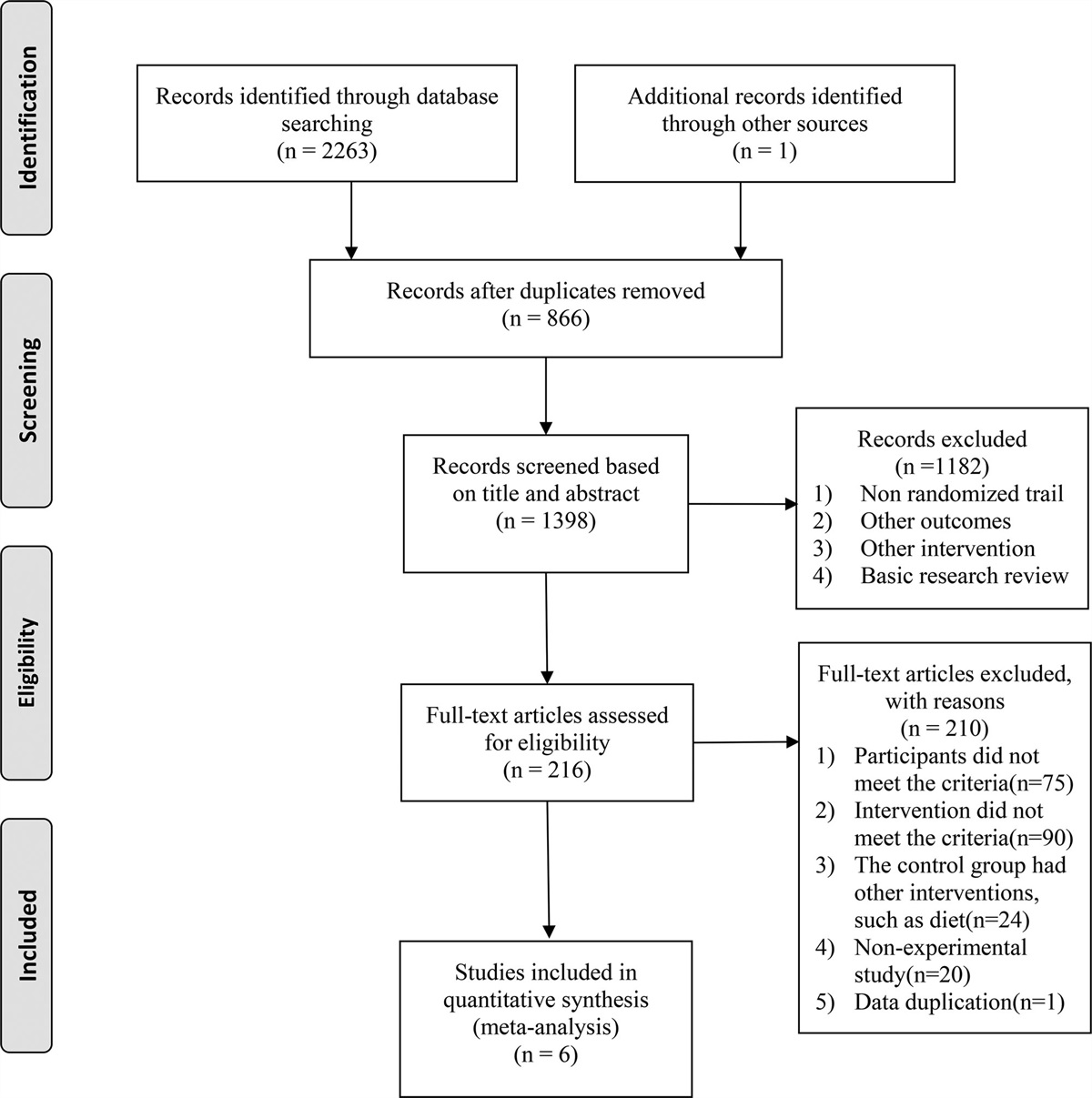
Methods Study designThe consensus procedure was based on a literature review and rating of statements by an expert panel (summarised in Fig. 1). Consensus statements were developed over the course of two online meetings and two rounds of voting. A meeting facilitator and medical writer attended the meetings and collated the results (Lumanity, UK).
 Fig. 1.: Consensus procedure flow chart. †Pilot statements and revisions are listed in Supplemental digital content 1, https://links.lww.com/EJGH/A950.
Fig. 1.: Consensus procedure flow chart. †Pilot statements and revisions are listed in Supplemental digital content 1, https://links.lww.com/EJGH/A950.The steering committee, comprising two experienced gastroenterologists and a general practitioner with a specialist interest in gastroenterology, defined key themes for literature searches and selected eight further panel members (five gastroenterologists and three primary care doctors) who were experienced in the management of reflux-like symptoms (average 28 years in practice, range 13–45 years), and involved in gastroenterology research and education (held positions in national/regional gastroenterological societies and/or have previously been involved in guideline development). The panel represented seven countries, including the USA, Italy, Spain, Greece, the Netherlands, Romania and the UK.
Targeted literature searchesLiterature searches using the PubMed database were conducted in June 2022 by an information specialist using keywords identified by the steering committee to identify relevant publications (excluding editorials, commentary, consensus statements, case reports, letters and response papers) in English from 2002 to 2022. The search strings for terms in the title and abstract are shown in Fig. 1. The terms 'infant', 'child', ‘eosinophilic oesophagitis’, 'Barrett’s', ‘functional dyspepsia’, ‘gastroparesis’, ‘oesophageal adenocarcinoma’ and ‘Burning Mouth Syndrome’ were excluded. The reference lists of retrieved articles were used to identify any further studies of interest. Throughout the consensus process, panel members were also encouraged to contribute supporting evidence.
Consensus procedureThe literature searches identified 406 articles. After the removal of 50 duplicates and the exclusion of nonrelevant studies, a total of 135 references were reviewed and used by the steering committee to develop 27 pilot statements around risk factors and interventions for reflux-like symptoms (Supplemental digital content 1, https://links.lww.com/EJGH/A950). The pilot statements and supporting articles were shared with the expert panel together with the level of supporting evidence for each study which had been assigned by the steering committee using the scale (1–6), as described previously [11] (Table 1). In the first consensus meeting, statements and evidence were reviewed and, based on panel discussion and agreement, three statements were added and four were eliminated (Supplemental digital content 1, https://links.lww.com/EJGH/A950). The revised pilot statements were then used as a basis for the steering committee to develop a set of 21 directive statements, which were shared (with supporting evidence) for anonymous voting using the Qualtrics online platform. For each statement, the experts, including the steering committee, indicated their level of agreement on a scale from 1 to 6 (1 = strongly disagree; 2 = disagree with major reservation; 3 = disagree with minor reservation; 4 = agree with major reservation; 5 = agree with minor reservation; and 6 = strongly agree). Results were analysed by the meeting facilitator. The consensus threshold was set a priori as agreement (level 5 or 6) by at least 67% of respondents.
Table 1. - Strength of evidence Level or GRADE Criteria Evidence 1+ Systematic review or meta-analysis of randomised controlled trials 1 Randomised controlled trial with adequate power 2+ Randomised controlled trial that does not meet level 1 criteria 3 Nonrandomised clinical trial or cohort study 4 Systematic review including observational studies, before-after studies, cross-sectional studies, cohort studies with non-contemporaneous controls, case-control study 5 Case series with controls 6 Case series without controls Recommendation A Supported by level 1 or 1+ evidence plus consensus B Supported by level 2 evidence plus consensus C Supported by level 3 evidence plus consensus D Any lower level of evidence plus consensus Grade High Further research is unlikely to change our confidence in the estimate of effect Moderate Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate Low Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate Very low Any estimate of effect is very uncertainDuring the second meeting, round one voting results were reviewed. Statements that did not reach consensus were discussed and revised and an additional statement was added ahead of a second round of voting. After the second round of voting, each of the consensus statements was assigned strength of evidence (A–D) by the steering committee and were rated using the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) system [12] (high, moderate, low, very low, see Table 1).
ResultsConsensus was achieved for 21 of the final 22 statements (Table 2). For each consensus statement, the result of the final vote and the grade of supporting evidence are given, followed by a discussion of key evidence. The statements have been separated into three categories of advice, (1) diet and exercise, (2) lifestyle and behaviour and (3) other interventions to target potential reflux-like symptom pathophysiology. The level of voting agreement achieved in each round is summarised in Figs. 2–4.
Table 2. - Consensus recommendations for the management of reflux-like symptoms Diet and exercise 1. Identification and avoidance of specific dietary triggers (e.g. citrus, tomatoes, highly spiced foods, fatty foods, fried foods and chocolate) should be recommended to individuals with postprandial reflux-like symptoms 2. Individuals who experience reflux-like symptoms after consuming alcoholic beverages should be advised to limit intake of alcoholic beverages 3. Individuals who experience reflux-like symptoms after consuming coffee should be advised to limit intake of coffee 4. Individuals who experience reflux-like symptoms after consuming carbonated beverages should be advised to limit intake of carbonated beverages 5. A low-fat diet should be recommended to individuals with reflux-like symptoms 6. Individuals with postprandial reflux-like symptoms should be advised not to overeat 7. Moderate, regular exercise should be recommended for overweight and obese individuals with reflux-like symptoms Lifestyle and behaviour advice 8. Individuals who experience reflux-like symptoms should be advised to avoid wearing items that are tight around their waist 9. Smoking cessation should be recommended to individuals with reflux-like symptoms who smoke tobacco products 10. Weight loss should be recommended to individuals with reflux-like symptoms who are overweight, obese or have recently gained weight 11. Head of the bed elevation should be recommended to individuals with night-time reflux-like symptoms 12. Sleeping in the left lateral decubitus position should be recommended to individuals with night-time reflux-like symptoms 13. Avoiding recumbence after meals and leaving a 3-hour interval between an evening meal and going to bed should be recommended to individuals with postprandial and/or night-time reflux-like symptoms Other interventions to target reflux-like symptom pathophysiology 14. Diaphragmatic breathing training is a treatment option for individuals with reflux-like symptoms, especially regurgitation 15. Stress management strategies should be recommended to individuals with reflux-like symptoms and stress 16. Brain-gut behavioural therapies (e.g. CBT or gut-directed hypnotherapy) should be recommended to individuals with reflux-like symptoms and signs of oesophageal hypervigilance and/or psychological distress 17. Disordered sleep is associated with an increased likelihood of having reflux-like symptoms 18. Alginate-antacid combinations are an effective treatment for reflux-like symptoms 19. Antacids are an effective treatment for reflux-like symptoms 20. Antacids and alginate-antacid combinations are an effective treatment option for reflux-like symptoms during pregnancy 21. Products containing hyaluronic acid and chondroitin sulphate are an effective treatment option for reflux-like symptoms Fig. 2.:
Fig. 2.: Breakdown of voting agreement for statements regarding diet and exercise advice for reflux-like symptoms.
 Fig. 3.:
Fig. 3.: Breakdown of voting agreement for statements regarding lifestyle and behaviour advice for reflux-like symptoms.
 Fig. 4.:
Fig. 4.: Breakdown of voting agreement for statements concerning other interventions to target reflux-like symptom pathophysiology.
Diet and exercise adviceStatement 1: Identification and avoidance of specific dietary triggers (e.g. citrus, tomatoes, highly spiced foods, fatty foods, fried foods and chocolate) should be recommended to individuals with postprandial reflux-like symptoms. Agreement: 100% (6, 63.6%; 5, 36.4%; grade of evidence: D; strength of recommendation: high).
Sixteen studies (one randomised crossover trial [13], one prospective cohort study [14], one before-after study [15], two case-control studies [16,17], eleven cross-sectional studies [18–28]) and two systematic reviews [29,30] supported the association of one or more dietary factors with reflux-like symptoms. The only study assessing a dietary intervention was a before-after study in patients presenting with reflux-like symptoms for the first time in primary care [15]. Reflux-like symptoms decreased significantly from baseline when patients were helped to identify and fully/partially eliminate dietary triggers, and 45% of patients agreed to continue symptom management with dietary intervention alone [15]. One cross-sectional study showing increased heartburn perception after ingestion of chili in patients with sleep disturbance (Pittsburgh Sleep Quality Index Score score >5) versus normal sleep [27], emphasizes how the impact of dietary triggers may be influenced by other lifestyle factors.
Statement 2: Individuals who experience reflux-like symptoms after consuming alcoholic beverages should be advised to limit their intake of alcoholic beverages. Agreement: 100% (6, 72.7%; 5, 27.3%; grade of evidence: D; strength of recommendation: high).
Seven studies (one RCT [31], one prospective cohort [14] and five cross-sectional [32–36]) and a meta-analysis [37] support a positive association between alcohol consumption and reflux-like symptoms. No interventional studies evaluating alcohol abstinence or reduction were identified. The meta-analysis by Pan et al. [37] found a linear association between alcohol consumption and gastro-oesophageal reflux disease (GORD; diagnosed by the presence of oesophagitis or symptoms), with erosive reflux disease having a stronger association compared with nonerosive reflux disease (NERD).
Statement 3: Individuals who experience reflux-like symptoms after consuming coffee should be advised to limit their intake of coffee. Agreement: 100% (6, 72.7%; 5, 27.3%; grade of evidence: C; strength of recommendation: moderate).
Five studies (two prospective cohort [14,38], two randomised crossover studies in coffee-sensitive individuals [39,40] and one cross-sectional study [41]) support a positive association between coffee consumption and reflux-like symptoms. However, a recent systematic review shows that the data are particularly conflicting, with multiple studies finding no increased risk of reflux-like symptoms in coffee drinkers [30]. We did not identify any interventional studies assessing the effect of reduced coffee intake on symptoms. However, substitution analysis in the cohort study conducted by Mehta et al. [38] showed that replacing two servings of coffee with water would reduce the risk of reflux-like symptoms [hazard ratio (HR), 0.96; 95% confidence interval (CI), 0.92–1.00] and a small, randomised study demonstrated significant symptom reduction and antacid use when coffee-sensitive individuals switched to dewaxed coffee (containing less caffeine and chlorogenic acids) [39].
Statement 4: Individuals who experience reflux-like symptoms after consuming carbonated beverages should be advised to limit their intake of carbonated beverages. Agreement: 100% (6, 72.7%; 5, 27.2%; grade of evidence: D; strength of recommendation: moderate).
Eight studies (two prospective cohort [38,42], one case-control [16], and five cross-sectional [22,24,33,41,43]) suggested that carbonated drinks are associated with an increase in reflux-like symptoms. The prospective cohort study conducted by Mehta et al. [38] reported an increased risk of reflux-like symptoms (HR, 1.29; 95% CI, 1.05–1.58; P < 0.0001) for those with the highest intake of soda (more than 6 servings/day) compared with the lowest intake (0 servings/day). Substitution analysis showed a reduced risk (HR, 0.92; 95% CI, 0.89–0.96) when 2 servings of soda were replaced with water. Two of the studies (one prospective cohort [42] and one cross-sectional [43]) found an association between carbonated beverage consumption and nocturnal reflux-like symptoms [42,43].
Statement 5: A low-fat diet should be recommended to individuals with reflux-like symptoms. Agreement: 90.9% (6, 63.6%; 5, 27.3%; grade of evidence: D; strength of recommendation: moderate).
Eight studies (one prospective cohort [14], one case-control [16] and six cross-sectional [22,24,25,43–45]) suggested that high dietary fat intake is associated with reflux-like symptoms and increased nocturnal reflux-like symptom severity. Three cross-sectional studies indicated that high saturated fat is an important risk factor [22,25,44], while a further cross-sectional study in an Albanian population [45], found that a predominantly non-Mediterranean diet (processed foods high in sugar, salt and saturated fats) was positively related to reflux-like symptoms versus a Mediterranean diet (frequent consumption of fresh fruit and vegetables, olive oil and fish) (adjusted OR, 2.3; 95% CI, 1.2–4.5). No interventional study assessing reflux-like symptoms after switching from a high-fat to a low-fat diet was identified.
Statement 6: Individuals with postprandial reflux-like symptoms should be advised not to overeat. Agreement: 100% (6, 81.8%; 5, 18.2%; grade of evidence: C; strength of recommendation: high).
One prospective cohort study supported overeating as a risk factor for reflux-like symptoms [14]. Multivariate regression analysis revealed that the habit of eating beyond fullness (continuing to eat beyond a sensation of fullness until unable to eat anymore) was a risk factor for reflux-like symptoms (OR, 2.85; 95% CI, 2.18–3.73). Symptomatic patients were defined as those with a reflux disease questionnaire score ≥12 and either a positive oesophageal endoscopy or a positive PPI test (>80% response to 2 weeks of PPI) suggesting acid-related aetiology was likely.
Statement 7: Moderate, regular exercise should be recommended to overweight and obese individuals with reflux-like symptoms. Agreement: 90.9% (6, 72.7%; 5, 18.2%; grade of evidence: D; strength of recommendation: high).
One case-control study [17] and five cross-sectional studies [19,21,46–48] provided evidence that lack of physical activity is a risk factor for reflux-like symptoms. Nilsson et al. [17] showed a linear association between increasing frequency of physical exercise sessions (e.g. running or swimming for at least 30 min) and reduced reflux-like symptoms (P value for linear trend 0.0001). Djärv et al. [48] suggested that physical exercise once a week for at least 30 min can significantly reduce the risk of reflux-like symptoms, while Eslami et al. [21] suggested that regular physical exercise for more than 2 h per week will reduce the risk of symptoms.
Lifestyle and behaviour adviceStatement 8: Individuals who experience reflux-like symptoms should be advised to avoid wearing items that are tight around their waist. Agreement: 90.9% (6, 18.2%; 5, 72.7%; grade of evidence: C; strength of recommendation: low).
One prospective cohort study found ‘wearing tight girdles or corsets’ to be among the most robust risk factors for reflux-like symptoms on multivariate analysis (OR 2.19; 95% CI: 1.42–3.38) [14].
Statement 9: Smoking cessation should be recommended to individuals with reflux-like symptoms who smoke tobacco products. Agreement: 100% (6, 100%; grade of evidence: D; strength of recommendation: high).
Seventeen studies (one prospective cohort [14], one case-control [17] and 15 cross-sectional studies [19,23,26,32,33,35,43,46,47,49–54]) and a meta-analysis [55] provided evidence that smoking tobacco products is a risk factor for reflux-like symptoms. A further population-based cohort study [56] found that cessation of daily tobacco smoking was associated with improvement in reflux-like symptoms among individuals within the normal range of BMI (OR, 5.67; 95% CI, 1.36–23.64), but not among overweight individuals.
Statement 10: Weight loss should be recommended to individuals with reflux-like symptoms who are overweight, obese or have recently gained weight. Agreement: 100% (6, 100%; grade of evidence: C; strength of recommendation: high).
Seven studies (one nonrandomised controlled trial [57], five cohort studies [58–62] and a case-control study [63]) demonstrated that weight loss has benefits for controlling reflux-like symptoms and discontinuation of PPI. The population-based nord-trøndelag health study study demonstrated a dose-dependent association between weight loss and reduced reflux-like symptoms (P value for trend P < 0.001), with the odds of symptom loss increasing four-fold (OR, 3.95; 95% CI, 2.03–7.65) in participants on medication who achieved a decrease in BMI of >3.5 units versus <0.5 units [59].
Statement 11: Head-of-the-bed elevation should be recommended to individuals with night-time reflux-like symptoms. Agreement: 100% (6, 72.7%; 5, 27.2%; grade of evidence: C; strength of recommendation: high).
Five systematic reviews [64–68] and five studies (two randomised crossover [69,70] two before-after [71,72] and one cross-sectional [46]) concluded that head-of-the-bed elevation may reduce oesophageal acid exposure and reflux-like symptoms. Methods used to raise the head-of-the-bed included wooden blocks (20 cm) [69,71], a 20 cm height/20-degree foam wedge pillow [70] and a positional device [72] (elevating the head/torso to 15 to 20 degrees together with maintaining left-side positioning).
Statement 12: Sleeping in the left lateral decubitus position should be recommended to individuals with night-time reflux-like symptoms. Agreement: 81.8% (6, 27.2%; 5, 54.6%; grade of evidence: B; strength of recommendation: moderate).
A systematic review [65] and two studies (one randomised sham-controlled [73] and one before-after study [72]) concluded that left lateral decubitus positioning has benefits for reducing nocturnal gastro-oesophageal reflux symptoms. Further studies have demonstrated significantly shorter acid exposure and clearance times in the left lateral versus right lateral and supine positions [74,75].
Statement 13: Avoiding recumbence after meals and leaving a 3-hour interval between an evening meal and going to bed should be recommended to individuals with postprandial and/or night-time reflux-like symptoms. Agreement: 100% (6, 81.8%; 5, 18.2%; grade of evidence: B; strength of recommendation: Moderate)
Three studies (one randomised crossover [76], one case-control [77] and one cross-sectional [46]) supported this statement. The randomised crossover study [76] demonstrated significantly greater supine acid reflux following a standardised meal consumed late in the evening (2 h before bed) compared with earlier in the evening (6 h before bed), especially in overweight patients, although no significant difference in symptom score was detected. The matched case-control study found that the odds of reflux-like symptoms increased seven-fold in patients whose dinner-to-bed time was less than 3 h versus an interval of 4 h or more (OR, 7.45; 95% CI, 3.38–16.4) [77], and the cross-sectional study showed that dinner within 2 h of going to bed was significantly associated with reflux symptoms (adjusted OR, 6.98; 95% CI, 5.36–9.08) [46].
Other interventions to target reflux-like symptom pathophysiologyThe initial focus of the consensus procedure was to evaluate interventions for reflux-like symptoms beyond acid reduction/neutralisation strategies. However, an antacid statement was included at the second round of voting to acknowledge its role in the self-management of symptoms.
Statement 14: Diaphragmatic breathing training may reduce reflux-like symptoms. Agreement: 81.8% (6, 27.2%; 5, 54.6%; grade of evidence: B; strength of recommendation: moderate).
A systematic review [78] and five studies (three randomised controlled pilot studies [79–81], one nonrandomised controlled study [82] and one case-control study [83]) provided evidence that diaphragmatic breathing has benefits for patients with reflux-like symptoms, including symptom reduction [79,81,82], increased lower oesophageal sphincter pressure/crural diaphragm tension [81,83], reduced reflux/acid reflux [79,80], improved quality of life [79,82,83] and reduced use of acid suppression medication [79,81].
Statement 15: Stress management strategies should be recommended to individuals with reflux-like symptoms and stress. Agreement: 100% (6, 54.6%; 5, 45.4%; grade of evidence: D; strength of recommendation: low).
Only one nonrandomised controlled study [84] was identified assessing the effectiveness of mindfulness-based stress reduction in PPI-treated patients with reflux-like symptoms reporting symptoms of depression or distress. Self-help mindfulness training significantly improved symptoms, overall health-related quality of life, and reduced levels of depression after 3 months compared with PPI alone (all P < 0.001).
Statement 16: Brain-gut behavioural therapies (e.g. cognitive behavioural therapy or gut-directed hypnotherapy) should be recommended to individuals with reflux-like symptoms and signs of oesophageal hypervigilance and/or psychological distress. Agreement: 90.9% (6, 72.7%; 5, 18.2%; grade of evidence: D; strength of recommendation: low).
Two before-after studies [85,86] have assessed brain-gut behavioural therapies in patients with upper gastrointestinal GI symptoms (functional heartburn [86] and supragastric belching [85]). The study in patients with functional heartburn found that weekly oesophageal-directed hypnotherapy sessions for 7 weeks were associated with a significant decrease in visceral anxiety and symptom severity, a significant increase in emotional quality of life, and a trend for reduced heartburn catastrophizing [86]. The study in patients with supragastric belching found that cognitive behavioural therapy (CBT; 4 sessions, as described previously [87]) showed significant reductions in acid exposure time and symptoms [85], which was maintained for 6–12 months after the completion of CBT [88].
Statement 17: Disordered sleep is associated with an increased likelihood of having reflux-like symptoms. Agreement: 72.7% (6, 45.5%; 5, 27.3%; grade of evidence: C; strength of recommendation: low).
Two cross-sectional studies indicated an association between poor sleep quality and reflux-like symptoms [52,89]. Three interventional studies (two small randomised controlled crossover studies [90,91] and one before-after study [92]) indicated that sleep deprivation may be hyperalgesic by demonstrating greater acid exposure and increased acid perfusion sensitivity score on the day following a night of disturbed sleep [90–92].
Statement 18: Alginate-antacid combinations are an effective treatment for reflux-like symptoms. Agreement: 100% (6, 90.9%; 5, 9.1%; grade of evidence: A; strength of recommendation: high).
Alginates form a buoyant precipitate on top of gastric contents creating a physical barrier to reflux. Seven RCTs have demonstrated symptomatic relief with alginate formulations versus placebo [93–100] and antacid alone [93,95,101], and one RCT suggested that alginate-antacids reduce night-time symptoms in PPI-treated patients [98]. Three meta-analyses of RCTs confirmed alginates are more effective than placebo (relative benefit increase up to 60% versus placebo [102]) or antacid alone for treating reflux-like symptoms [102–104] and three studies suggested noninferiority to omeprazole [94,105,106].
Statement 19: Antacids are an effective treatment for reflux-like symptoms. Agreement: 90.9% (6, 45.5%; 5, 45.5%; grade of evidence: A; strength of recommendation: moderate).
Most antacid research was conducted before the 2002 cut-off point for the current literature search. A meta-analysis of these RCTs reported an 11% relative benefit increase compared with placebo [102]. Two randomised, controlled, crossover studies conducted more recently demonstrated that a calcium carbonate gum [107] and hydrotalcite (aluminium hydroxide, magnesium hydroxide and carbonate) chewable tablets [108] effectively reduce heartburn.
Statement 20: Antacids and alginate-antacid combinations are an effective treatment option for reflux-like symptoms during pregnancy. Agreement 90.9% (6, 45.5%; 5, 45.5%; grade of evidence: B; strength of recommendation: high).
Antacids and alginate-antacids are considered safe in pregnant and breastfeeding women as they are not systemically absorbed and have a long history of clinical use [109], although formulations with sodium bicarbonate as the main active ingredient are generally avoided given the potential for metabolic alkalosis [110]. Three studies (one RCT [111] and two-phase IV studies [112,113]) reported reduced frequency and intensity of heartburn in pregnant women, without any treatment-related adverse events or changes in serum sodium.
Statement 21: Products containing hyaluronic acid and chondroitin sulphate are an effective treatment option for reflux-like symptoms. Agreement: 81.8% (6, 82%; 5, 18%; grade of evidence: B; strength of recommendation: low).
Bioadhesive formulations target reflux-like symptoms by directly protecting the oesophageal mucosa. One RCT [114] two pilot RCTs [115,116] and an exploratory postmarketing study [117] have demonstrated symptom reduction with several different formulations in patients with reflux-like symptoms. Two formulations were assessed in RCTs, one consisted of hyaluronic acid, amino acids and rice extract [115] and the other, hyaluronic-chondroitin sulphate [114,116]. Both demonstrated reflux-like symptom reduction versus placebo in NERD patients.
A statement regarding natural remedies [some natural remedies (aloe vera, amla or apple cider vinegar) may have benefits for reflux-like symptoms] failed to reach consensus after the second round of voting, with only 36.4% voting agreement at level 5 or 6 (Fig. 4). The supporting evidence from three RCTs [118–120] was considered weak, and the expert group was not able to share any clinical experience of efficacy for such products.
DiscussionGORD and dyspepsia management guidelines, such as the recently updated American College of Gastroenterology guidelines [121], generally include lifestyle recommendations as a first approach for symptomatic patients, but they are not always implemented in practice. This Delphi-style process builds on the published recommendations by providing greater analysis of the published evidence combined with clinical experience, with the goal of developing education for providers and patients. Consensus was achieved for 21 statements according to the prespecified criteria (67% voting either ‘strongly agree’ or ‘agree with minor reservation’). Eleven statements achieved the strongest (100%) agreement; five are related to diet and include identification and avoidance of dietary triggers, limiting alcohol, coffee and carbonated beverages, and advising patients troubled by postprandial symptoms not to overeat. The remaining six statements with 100% consensus concern advice around smoking cessation, weight loss, raising the head-of-the-bed, avoiding recumbency after meals, stress reduction and alginate use.
The wording of the consensus statements regarding food and beverage advice reflects the fact that dietary risk factors are highly individualised, which is often not emphasised in guidelines and patient brochures. Even for a given individual, the ability of dietary factors to trigger symptoms may depend on other factors, such as sleep disturbance or stress, which have the potential to increase symptom perception. A statement on tea drinking was not included based on the findings of a meta-analysis suggesting no overall relationship with GORD [122]. However, the amount and type of tea drunk worldwide is highly variable and stratification by geographical region suggests that it may be a more important risk factor in Eastern Asia [29,122].
Advising patients not to overeat was given 100% consensus, even though the evidence is sparse [14] and no interventional
Comments (0)