Cancellation of elective surgeries is a key indicator of healthcare quality, with significant implications for both patient care and hospital management. Not only it does reflect inefficiencies in hospital operations but also it carries substantial cost implications and adversely affects patient satisfaction.
4.1 Overall cancellation rate and comparison to literature
This study revealed that the overall same-day elective surgery cancellation rate at El-Demerdash University Hospital was 12.59%. This rate is notably lower than that reported in a comparable Egyptian study by El Bokl et al. (2021) at the Cardiothoracic Ain-Shams University Hospital, which recorded a cancellation rate of 21.7% [15]. The latter hospital is a highly specialized facility that manages complex patients and procedures, which likely contributes to its higher cancellation rate, in addition to its practice of preparing standby patients in anticipation of possible cancellations [15]. The cancellation rate observed in the current study was also lower than that reported in several other low- and middle-income countries. For instance, in India, a large multidisciplinary government hospital reported a same-day cancellation rate of 17.6% [27]. One possible explanation for this discrepancy is the difference in scheduling systems: in the Indian study, operative lists were finalized at 14:00 the day before surgery, whereas in our study, final lists were submitted at 7:00 a.m. on the same day, potentially allowing for more up-to-date decision-making and fewer cancellations. In other developing countries, the rates were even higher: 18.45% in Ethiopia [28], 21.41% in Brazil [29], and 48.5% in Nigeria [30]. The high rates in Ethiopia and Nigeria may reflect limitations in healthcare infrastructure and resource availability. Overall, surgical cancellations are complex and multifactorial, with discrepancies influenced by differences in patient populations, case complexity, hospital settings, and operating room management practices [13, 28].
Conversely, the cancellation rate reported in this study exceeds the commonly cited efficiency benchmark of approximately 5% [7, 31]. It also exceeds the rates observed in Jordan (3.6%) [33] and high-income countries, including Hong Kong (7.6%) [10], Saudi Arabia (11.1%) [32], and the UK (1.1%) [34]. According to Schuster et al. (2011), university hospitals tend to have higher cancellation rates than smaller hospitals due to less predictable workflows, the demands of teaching environment, higher patient loads, and greater complexity of cases [35]. As a major tertiary referral center serving multiple surgical specialties, El-Demerdash University Hospital shares these characteristics, which may explain its relatively high cancellation rate. Interestingly, the observed cancellation rate closely matched the perceptions of most OR staff interviewed in the qualitative component of this study. Most staff estimated a cancellation rate between 10 and 20%, while anesthesiologists tended to estimate lower rates (less than 5%), likely due to varying interpretations of what constitutes a cancelled surgery. Specifically, many staff members considered a surgery “cancelled” only if the patient had already arrived at the operating department, reflecting a possible misconception about the broader definition of surgical cancellation.
4.2 Key demographic and departmental insights
Identifying the demographic groups most affected by cancellations can help guide targeted improvement efforts. In the current study, the mean age of patients was 40.5 years (± 19.49), with age showing a statistically significant difference between cancelled and non-cancelled cases. The highest cancellation rates were observed among seniors (aged 65 and older), likely due to their higher prevalence of comorbidities and increased need for postoperative ICU beds. This finding aligns with a study from a Korean university hospital, where 21% of surgeries in patients aged 60 or older were cancelled [36].
The current study also revealed significant differences in cancellation rates between surgical departments. Vascular surgery had the highest cancellation rate (25.40%), followed by plastic surgery (16%) and urology (14.53%). The high rate in the vascular department may be attributed to the medical complexity of patients, the higher proportion of elder patients, and a shortage of dedicated operating rooms, as only 1 out of 21 ORs was allocated for vascular surgeries. This contrasts with findings from a study in the UK, where the highest cancellation rates were observed in the ENT and general surgery departments, largely due to secretarial scheduling practices [37]. Notably, pain management experienced zero cancellation, possibly because these are performed solely by anesthetists, streamlining the process. An alternative explanation could be the small sample size of pain management cases included in this study.
4.3 Vital few causes of surgical cancellations
Hospital-related factors accounted for the majority of cancellations (71.31%), followed by patient-related factors (25.58%). This finding is consistent with two systematic reviews, both of which identified hospital-related reasons as the most common cause of surgical cancellations [28, 38].
Regarding the OR staff’s expectations of the most common causes of cancellation, about half reported unavailable ICU bed as the leading cause of elective surgery cancellations. The quantitative analysis, however, identified this as the second most frequent cause, with changes in the patient’s medical condition ranking third. A few staff members attributed cancellations to patient-related factors, such as illiteracy. Although the hypothetical causes align with the findings of the quantitative study, none of the staff mentioned the actual leading cause “unavailable OR time.” Furthermore, the order of perceived causes did not match the actual rankings found in the data.
The most frequent hospital-related cause was unavailable OR time, responsible for 24.03% of cancellations. This could be due to various reasons, including anesthetic restrictions (e.g., a 3 p.m. cutoff for major surgeries), overscheduling, and prolonged previous operations. Similar findings were reported in a study from India, where 78% of cancellations were attributed to OR time constraints due to anesthetic restrictions [39]. Another study in Spain reported that 22.5% of cancellations were caused by a lack of OR time [40].
The qualitative findings from this study provided deeper insights into this issue. Many staff members attributed prolonged surgeries to intraoperative complications, the involvement of trainee surgeons, or inefficient time management. While surgeons often viewed the 3 p.m. anesthesia cutoff as a limiting constraint, anesthesiologists generally considered it a necessary safeguard to avoid overrunning scheduled hours.
In teaching hospitals such as El-Demerdash, surgeries often take longer due to the involvement of trainees, which contributes to surgical list overruns—a common challenge faced by academic institutions worldwide [37, 41]. Key strategies to reduce cancellations stemming from this issue include optimizing OR scheduling by adopting clear scheduling criteria and implementing mathematical modeling-based algorithms. Ensuring that all cases undergo preoperative anesthesia assessment and aligning surgical lists with available resources— such as staff, ICU beds, and equipment—are also essential. Emphasis should be placed on effective time management, particularly ensuring a timely start of the first case. Additionally, it is important to re-evaluate the 3:00 p.m. anesthesia cut-off policy, considering its advantages and drawbacks. Finally, linking staff incentives to performance in reducing cancellations and improving workflow efficiency may contribute to sustained improvements. The second most common cause of cancellation was the unavailability of ICU beds, accounting for 21.71% of all cancellations. Qualitative findings suggested several contributing factors: ICU bed availability was often confirmed on the same day of surgery, multiple complex cases requiring postoperative ICU care were sometimes scheduled on the same list, and poor communication between surgical, anesthetic, and ICU teams. Although our data cover only a specific data collection period, this issue appears to be ongoing rather than seasonal, likely reflecting the hospital’s status as a major tertiary referral center that handles a high volume of complex surgical cases each month. A UK study found that 66% of surgical cancellations in a teaching hospital were due to bed shortages, exacerbated by emergency admissions and medical patients requiring critical care [42].
In contrast, a study from Spain reported that cancellations due to bed shortages were rare, thanks to efficient preoperative planning and flexible bed allocation [40]. In our setting, suggested solutions include the following: improving interdepartmental, establishing clear criteria for postoperative ICU bed requests, using conventional or artificial intelligence (AI)-based prediction models to anticipate ICU needs, and increasing the number of dedicated ICU for elective cases.
Changes in the patient’s medical condition accounted for 14.73% of cancellations and were the leading cause among patient-related factors. These cancellations may have resulted from discrepancies between the preoperative assessments conducted the day before surgery and the clinical evaluations made by the operating room team on the day of surgery. A similar issue was reported in Spain, where 50% of cancellations were due to medical deterioration between the preoperative check and the operation [40]. Strategies to tackle this issue include providing counseling and education to reduce pre-surgical anxiety, ensuring adherence to medication and vital sign monitoring, and aligning anesthesia staffing levels with the surgical schedule to allow for comprehensive patient assessments. Additionally, optimizing the time between assessment and surgery may improve the accuracy of preoperative fitness assessments, especially for high-risk patients (ASA ≥ 3). Regular interdisciplinary meetings are also recommended to develop evidence-based policies aimed at reducing cancellations.
Unavailable or failed equipment contributed to 7.75% of cancellations, with a striking 60% of these cases occurring in the urology department. This issue was attributed to limited hospital resources, outdated equipment, and errors by external vendors responsible for providing specialized surgical tools. Equipment-related cancellations were also observed in other studies—for instance, a 4.2% equipment-related cancellation rate was documented in Saudi Arabia [43], while the UK reported a much lower rate of 0.4% [44]. To reduce such cancellations, implementing a comprehensive checklist to verify the availability and functionality of required equipment as part of the preoperative preparation process is strongly recommended. Furthermore, establishing contracts with reliable suppliers committed to delivering high-quality, timely equipment, along with continuous supplier evaluation, can significantly minimize the risk of last-minute equipment failures or shortages. Ensuring accountability and consistency in the surgical supply chain is essential for improving operating room efficiency and patient safety.
4.4 Successful stories
A quality improvement project at a large tertiary care children’s cancer center in Riyadh, Saudi Arabia, succeeded in reducing operating room cancellations by 17%, lowering the rate from a baseline of 22% through a series of targeted interventions. A daily OR huddle was implemented to identify critical areas requiring intervention. These included personalized medical planning, pre-anesthesia evaluations, specialized consultations, and coordination of blood product support. Improvements in communication were also central to the project’s success, incorporating patient and nurse education, re-evaluation protocols, and a preoperative checklist review to ensure a 24-h cancellation notice to the OR scheduling team [45].
4.5 Strengths and limitations
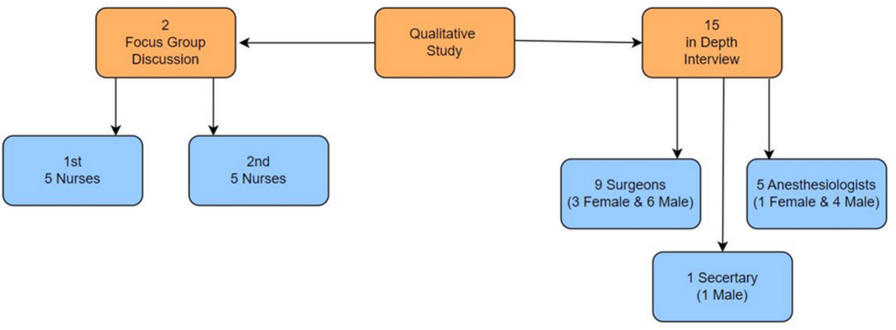
This study has several limitations. First, the study employed a cross-sectional design, which is appropriate for measuring prevalence but does not establish causality. Second, the study was conducted in a single, large surgical tertiary hospital (El-Demerdash Hospital), which may limit the generalizability of findings to other healthcare settings with different contexts. To enhance generalizability, future research in diverse hospitals and regions is recommended. Third, the use of convenience sampling may introduce selection bias. Although random sampling would provide more valid, generalizable results, it was not feasible in the current study where operative lists are generated day by day. However, measures were taken to minimize selection bias, as detailed in the sampling section. Moreover, surgical classifications were based on the hospital’s financial categorization rather than purely clinical distinctions. Additionally, the ASA classification scores were calculated only for cancelled cases, preventing direct comparison between cancelled and non-cancelled cases regarding that factor. No data were available on whether patients attended the anesthesia clinic, which limited the ability to assess any correlation between preoperative anesthesia evaluation and cancellations due to changes in the patient’s medical condition. Despite these limitations, the study has several notable strengths. The mixed-methods design provided a comprehensive understanding of the problem by integrating quantitative data with in-depth qualitative insights. Moreover, the large sample size enhanced the statistical robustness, and the prospective nature of data collection helped ensure its accuracy.





Comments (0)