Research ethics approval to conduct this historical cohort study was obtained from the Western University Research Ethics Board (REB: 00000940; approved 4 November 2019; London, ON, Canada) with a waiver for informed consent.
Study design and data sources
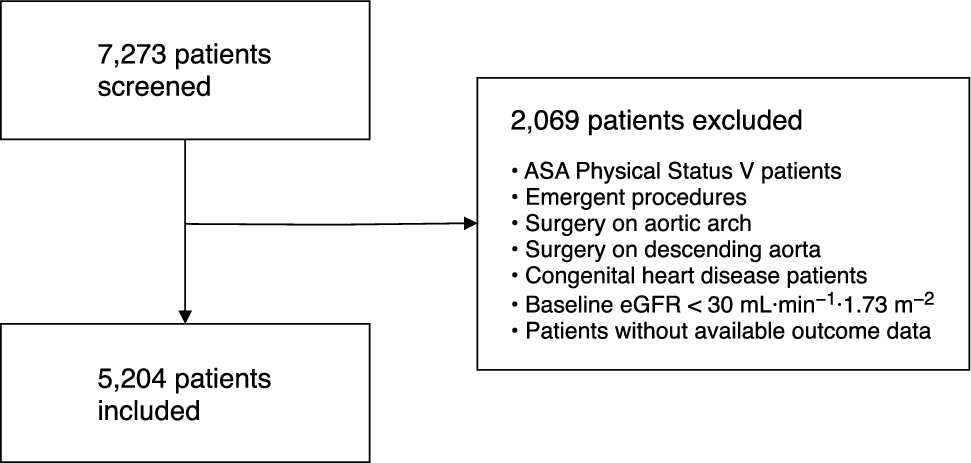
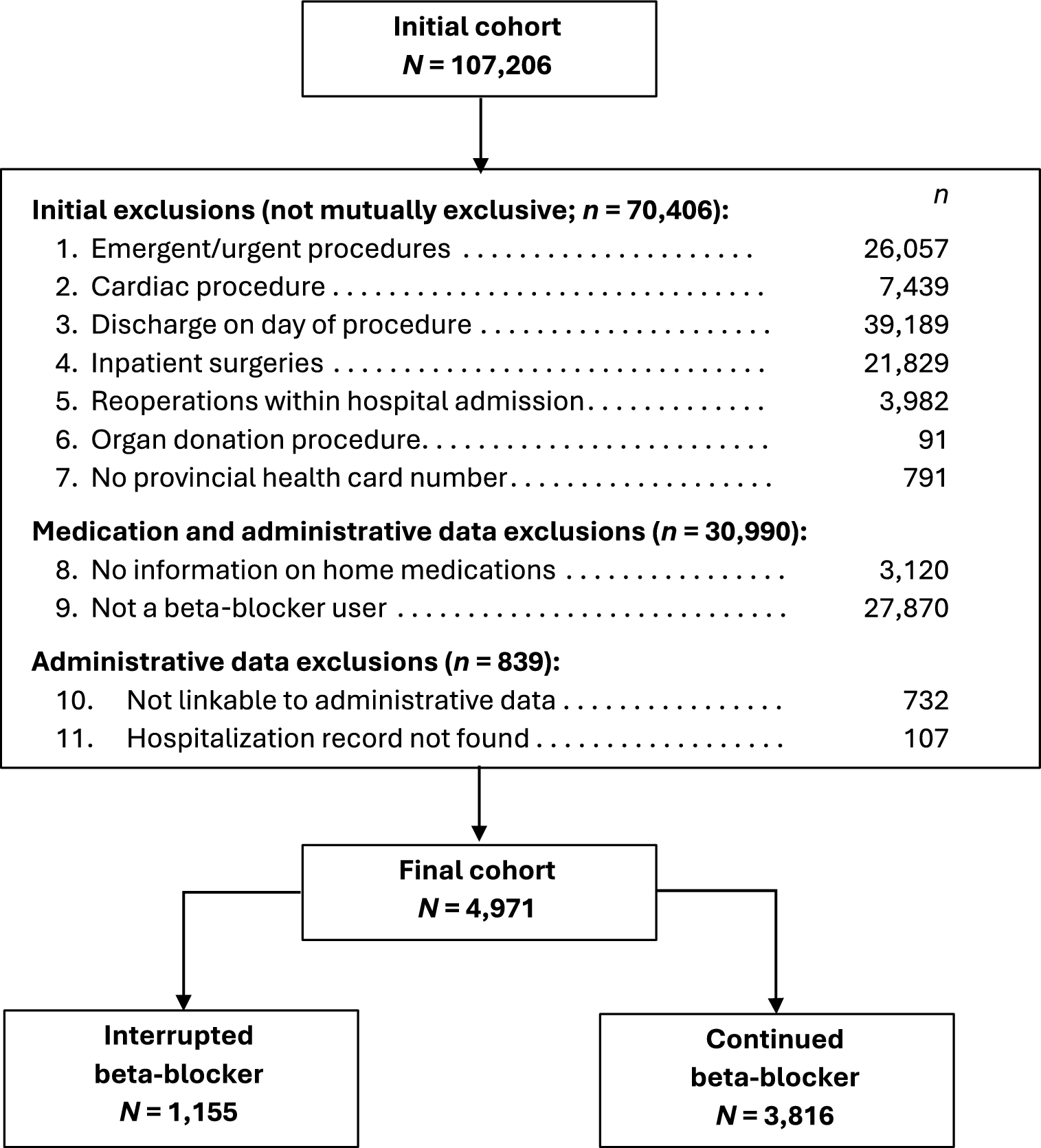
We identified the initial study cohort using the operating room booking system at two large academic hospitals to capture all consecutive surgical procedures scheduled for patients 18 yr and older from 1 May 2014 to 31 December 2018. The two recruiting hospitals (University Hospital and Victoria Hospital, London Health Sciences Centre, London, ON, Canada) are part of a single institution located in southwestern Ontario and one of Canada’s largest acute care teaching hospitals (approximately 40,000 admissions per year). All elective patients undergoing noncardiac surgery and admitted for at least one night postoperatively were eligible for inclusion. We excluded patients who underwent emergency surgery, organ donation procedures, one-day-stay surgery, or operation/reoperation during an inpatient admission. We also excluded patients who did not have a provincial health card number, if information on home medication was missing from the patient’s electronic medical record (EMR), or if they did not have an active prescription for a beta-blocker medication.
Data collected from the institution were transferred to ICES (formerly the Institute for Clinical Evaluation Sciences; headquarters: Toronto, ON, Canada)10 for deterministic linkage using an encrypted identifier to administrative data holdings and statistical analysis. Residents of Ontario have access to universal health care coverage, and administrative databases contain information relating to all insured hospital and physician-based services. We used administrative data sets in the current study to capture additional baseline variables and study outcomes, and Electronic Supplementary Material (ESM) eTable 1 provides a complete list of the data sets used to conduct this study. Following transfer of the project data set to ICES, we excluded patients if we were not able to link them to the administrative data holdings on the basis of their health card number or if we did not find an aligning hospitalization record.
Variable definitions
We obtained information about home medication prescriptions, including acute medication interruption (i.e., whether or not the patient continued their prescribed medication on the morning of surgery), from the hospitals’ EMR. This information included the date and time of the last dose of all prescribed home medication, as obtained by the preoperative care nurses. The hospital EMR also documented the date and time of the first dose of all postoperative medications given in hospital. This allowed us to determine the exact timing of preoperative beta-blocker interruption. The primary exposure, beta-blocker interruption, was defined as not taking beta-blocker medication on the morning of surgery. We also used the EMR to capture patient demographics (including age, sex, and body mass index), as well preoperative hemoglobin and creatinine levels (used to calculate estimated glomerular filtration rate),11 categorization according to the American Society of Anesthesiologists (ASA) Physical Status classification system, and occurrence of a preadmission clinic nurse visit, anesthesiology consultation, or internal medicine consultation. Electronic medical record data also captured procedure-related information such as operative duration and type of anesthesia used, blood transfusion during admission, postoperative in-hospital medication prescriptions, laboratory diagnostics, in-hospital consultation of the critical care outreach team, life-threatening medical emergencies (code blue), and intensive care admissions.
Administrative data holdings contributed information on rural residence, neighbourhood income quintile (adjusted for household size and housing costs), hospitalizations and emergency department (ED) visits in the previous year, and calculation of the Charlson Comorbidity Index score (based on hospitalizations from the previous 5 years). We used a combination of both EMR and administrative data to capture history of specific comorbid conditions (including diabetes mellitus, hypertension, ischemic heart disease, congestive heart failure, atrial fibrillation, cerebrovascular disease, peripheral vascular disease, chronic kidney injury, and chronic obstructive pulmonary disease), as well as calculation of the Revised Cardiac Risk Index (RCRI) score (ESM eTable 2).12
The primary outcome was 30-day all-cause mortality, and we also investigated 90-day and 1-year mortality. In-hospital outcomes, reflecting events occurring from the time of surgery to hospital discharge, included myocardial ischemia, nonfatal cardiac arrest, acute kidney injury or new onset dialysis, and intensive care unit (ICU) admission. Outcomes captured up to thirty days after surgery included myocardial infarction, cardiac revascularization, chronic heart failure, atrial fibrillation, ischemic stroke, hospital readmission, and emergency department visit. We also investigated two composite outcomes, one for in-hospital outcomes and the other for 30-day outcomes, that included myocardial infarction, cardiac arrest (in-hospital composite only), cardiac revascularization, congestive heart failure, and atrial fibrillation. Electronic Supplementary Material eTable 3 provides all of the codes used to capture study baseline and outcome variables from administrative data holdings.
Statistical analysis
We evaluated between-group differences in baseline characteristics using standardized differences. For large data sets, standardized differences are often preferred over P values owing to the impact of sample sizes on probability tests. A standardized difference greater than 0.10 can be interpreted as a potentially meaningful between-group difference.13
We used unadjusted and adjusted logistic regression models to evaluate the association between beta-blocker interruption and each of the study outcomes. We did not investigate adjusted models for secondary outcomes with a small number of events (< 40 events in either group). Regression models included the following covariates: patient age, sex, RCRI score, preadmission anesthesiology or internal medicine consultation, blood transfusion, and a propensity score predicting beta-blocker interruption. We calculated the propensity score using a logistic regression model and included all of the baseline variables listed in ESM eTable 4, except for those directly related to or occurring after exposure and those representing a combination of other included variables (e.g., we did not include RCRI score in the propensity score, but each of the RCRI components were individually included). Using this same propensity score, we also conducted post hoc sensitivity analyses using inverse probability of treatment weighting (IPTW) using weight stabilization and truncating weights at the 1st and 99th percentiles. We investigated a weighted baselines table to confirm balance on all included covariates (defined as a standardized difference < 0.10). We used robust sandwich variance estimators to create weighted logistic regression models and included the same covariates as in the primary analysis. For the primary outcome, we also investigated a sensitivity analysis in which beta-blocker interruption was modeled as a continuous variable representing the total beta-blocker-free period. We included all patients in this analysis, regardless of when the interruption began. Further, we tested whether preoperative interruption of other cardiac medications (calcium channel blockers, angiotensin-converting enzyme inhibitors [ACEIs] or angiotensin II receptor blockers [ARBs], statins, and platelet aggregation inhibitors) would affect postoperative outcomes. Due to ICES privacy requirements, we report values representing five or fewer patients as ≤ 5, while we report those that would allow recalculation of these values as not reportable (NR). For all analyses, reported P values are from two-tailed tests where we considered a value of < 0.05 statistically significant. We performed all analyses using SAS EG version 7.15 (SAS Institute Inc., Cary, NC, USA). Investigators had complete access to the study data. Reporting of this study follows the Reporting of Studies Conducted Using Observational Routinely-Collected Health Data (RECORD) statement.14



Comments (0)