Study design, setting, and data sources
We conducted a QI initiative supported by evaluation using a retrospective observational cohort and a quasi-experimental interrupted time series design. The setting was a multisite academic health sciences network (The Ottawa Hospital, Ottawa, ON, Canada) serving a catchment area of 1.5 million people. Our network includes two inpatient campuses (one specializing in complex orthopedic and surgical oncology, the other focusing on trauma, neurosurgery, and vascular surgery) with 40 operating rooms combined. The Ottawa Health Science Network Research Ethics Board waived the requirement for written informed consent, as this initiative used de-identified, routinely collected data for QI evaluation. We extracted data to support the initiative from our network’s EHR (EPIC, EPIC Systems, Verona, WI, USA), which records all relevant data from health care encounters (e.g., demographics, procedures, consults and assessments, and medications prescribed and dispensed). We included surgical patients that consulted our APS. We chose this cohort as the patients with the greatest degree of pain, who were likely to be prescribed pregabalin perioperatively. Additionally, our EHR interventions were able to be rolled out within an anesthesiology-specific context with much greater ease than across the entire hospital’s EHR. The intraoperative anesthesiologist determines when a patient is followed by our APS team and completes APS-specific orders. The orders can then be modified as clinically indicated by our APS providers, who include physician anesthesiologists with either fellowship training in pain management or individuals with a focused interest and expertise in acute pain management (~40 staff anesthesiologists). An advanced practice nurse supports the service on weekdays. Our APS order sets allowed only pregabalin to be ordered; gabapentin was reserved for patients already taking it at home. Given our system’s pre-existing preference for pregabalin in de novo APS orders, we focused exclusively on pregabalin in our QI initiative. Reporting followed the recommended EQUATOR guidance for observational and QI methodologies (Strengthening the Reporting of Observational Studies in Epidemiology [STROBE] and Standards for Quality Improvement Reporting Excellence [SQUIRE 2.0], respectively).
Study population
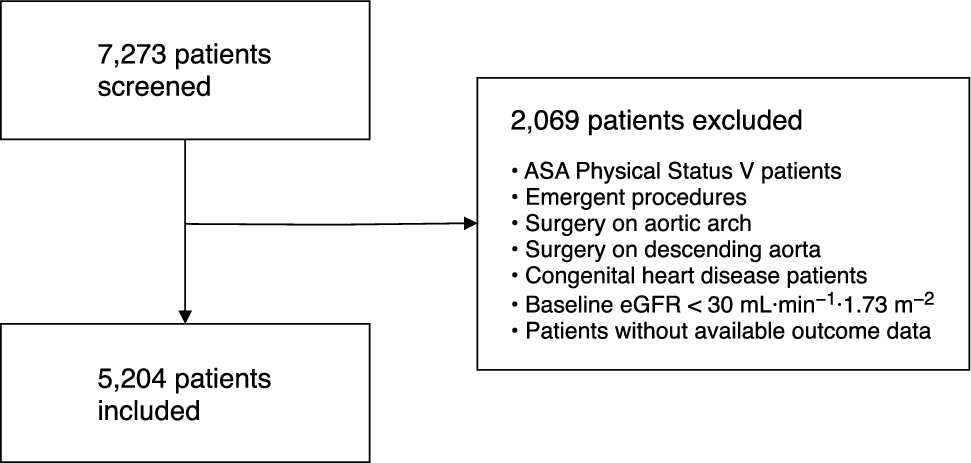
We identified all episodes of care (admission to APS) for adults (aged ≥ 18 yr) undergoing inpatient surgery between 19 January 2021 and 4 January 2023 and who were admitted to our APS. We chose this time frame to provide a stable baseline period of approximately 12 months and ensure adequate time periods after each change strategy was initiated (approximately 6 months after each). As an episode-based cohort, a patient could contribute more than one episode of care, however, our unit of analysis was not the patient or episode but instead was the weekly period.
Outcomes
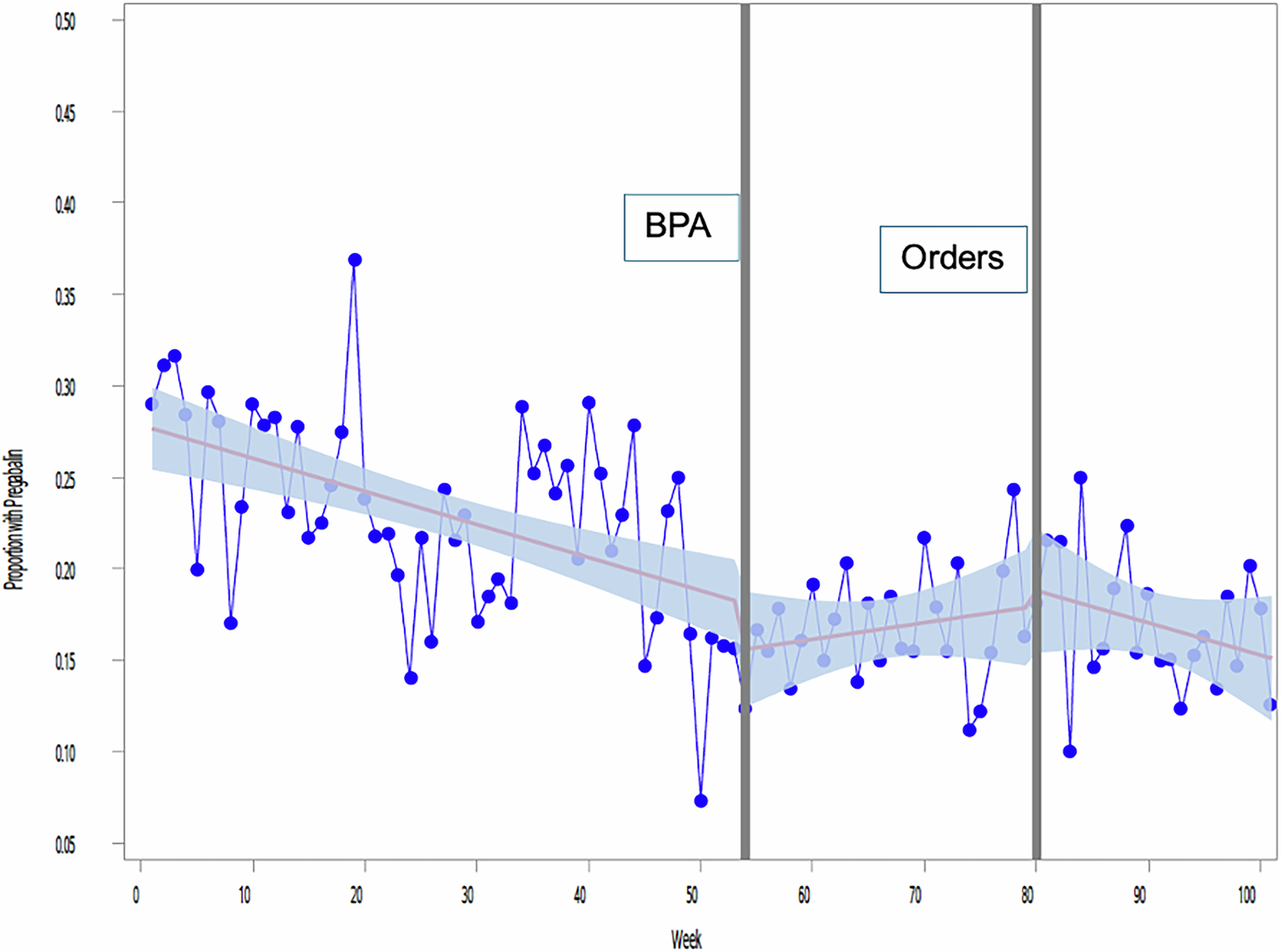
Our primary outcome was the proportion of patients prescribed pregabalin during their admission to our institution’s APS. This required that a prescription be placed, and the medication dispensed at any point between hospital admission and discharge. Our balancing measure aimed to identify unintended consequences to our EHR interventions, operationalized as the highest numeric rating scale (NRS; 0–10) pain score experienced by patients on postoperative day 1. We used nursing flowsheets to capture NRS scores.
Covariates
Patient-level data extracted to support cohort description included age, sex, surgical specialty, surgical urgency, anesthesia type, and American Society of Anesthesiologists (ASA) Physical Status score.
Interventions
To support a decrease in inappropriate pregabalin prescribing, we initiated two sequential interventions using our EHR. Intervention 1 was the initiation of a BPA warning, which was integrated into EPIC and went live on 19 January 2022. This BPA alerted prescribers of pregabalin’s increased risks for sedation or respiratory depression if selected for a patient on APS (at this time, pregabalin was available as a standard checkbox on our APS orders). The BPA appeared for every pregabalin order for an APS patient and included additional information regarding 5 specific risk factors for adverse respiratory events, as identified by a working group (6 anesthesiologists and 1 nurse) of our Quality and Patient Safety committee (age > 70 yr, history of obstructive sleep apnea, STOP-BANG score > 4, body mass index > 35 mg·kg−1, or concurrent ordering of a sedative or intravenous patient-controlled analgesic modality).7,11 Of note, our BPA could be bypassed as follows: 1) pregabalin is a home medication, 2) the dose was being increased or decreased, and 3) the ordering provider felt that the benefits outweighed the risks. Intervention 2 involved removing the pregabalin checkbox in our standardized APS order set (pregabalin could still be ordered, but a prescriber would need to choose the order from a formulary search) and went live on 19 June 2022. E-mail communication to all possible prescribers (anesthesiologists, anesthesiology residents, and anesthesiology fellows) conveying the changes and underlying rationale and evidence for the interventions supported these interventions. The only other structured activities related to pregabalin prescribing were not concurrent with either intervention, and did not alter the prescribing environment, but are reported for transparency and to support sensitivity analyses as follows: a morbidity and mortality rounds presentation occurred on 16 June 2021 where a case of respiratory arrest was discussed with pregabalin as a possible contributor; and a grand rounds presentation on 20 April 2022 that involved the discussion of recent evidence of gabapentinoids’ lack of effectiveness and possible harm.
Sample size
As we average approximately 100 APS admissions per week, we organized our study data into weekly time periods to support our segmented regression analyses (interrupted time series analysis), which we expected to provide more than the 40 measurements (APS admission) per period as required for a stable time series analysis. This would also provide us with 50 preintervention and 25 postintervention periods for each change strategy, which exceeds recommended minimums based on simulation studies.12
Statistical analysis
We computed descriptive statistics using mean (standard deviation [SD]) for normal, median [interquartile range (IQR)] for skewed, continuous data, and counts and proportions for categorical data. We compared the results across study phases (preintervention, postintervention 1 [January 2022], and postintervention 2 [June 2022]) using analysis of variance for continuous normal variables, Kruskal–Wallis test for continuous skewed variables, and Chi square tests for categorical variables.
We used segmented linear regression (PROC MIXED, SAS® version 9.4 for Windows, SAS Institute Inc., Cary, NC, USA) with restricted maximum likelihood estimation and an autoregressive covariance matrix to account for autocorrelation to estimate the association of intervention implementation and changes in quality outcomes and balancing measures.13,14 From this model, we estimated terms for preinterruption intercept, preinterruption slope, postintervention 1 level change, postintervention 1 slope change, postintervention 2 level change, and postintervention 2 slope change. Level changes estimate the immediate impact of the intervention, while slope changes estimate the trend over time after the intervention. We also estimated the total counterfactual effects (impact of postintervention pregabalin prescribing trends as compared with the prechange trend) using the delta method.15 For each parameter, we estimated the point estimate and 95% confidence interval (CI). While many interrupted time series analyses evaluate a single change, our model included terms for the second change, which meant that effect estimates for intervention 2 were appropriately adjusted for the effects of the intervention 1 strategy.16
Sensitivity analyses
We completed a sensitivity analysis that excluded our cesarean delivery population, as patients undergoing this procedure rarely received gabapentinoids. Next, although the primary assumption for a robust interrupted time series analysis requires no other concurrent interventions (a condition supported by our knowledge of practice within our network), we developed a segmented regression model that included interruptions corresponding to two rounds of internal presentations on gabapentinoid safety and efficacy. This model included four interruptions in total, for which we estimated both level and slope changes: BPA implementation, morbidity and mortality rounds, grand rounds, and removal of the pregabalin checkbox from the order set. We performed a post hoc sensitivity analysis to evaluate the robustness of the primary analysis (as proportions may not adhere to assumptions of linear regression because they are bounded at 0 and 1). For this analysis, we fit a beta regression model to our data to estimate the odds ratios (OR), which can be interpreted as the relative odds of pregabalin prescribing being higher (OR > 1) or lower (OR < 1) in one period than the previous period.



Comments (0)