
Remember me


The protocol for this single-centre, randomized, crossover trial was approved by the Institutional Review Board of Seoul National University Hospital (approval no. H-1711-094-901; 22 January 2018) before patient enrolment. This trial was registered at https://www.ClinicalTrials.gov (NCT05495880; first submitted 8 August 2022). Written informed consent was obtained from all participants before surgery. The study adhered to the principles of the Declaration of Helsinki and we followed the Consolidated Standards of Reporting Trials (CONSORT) guidelines for the preparation of this manuscript.13
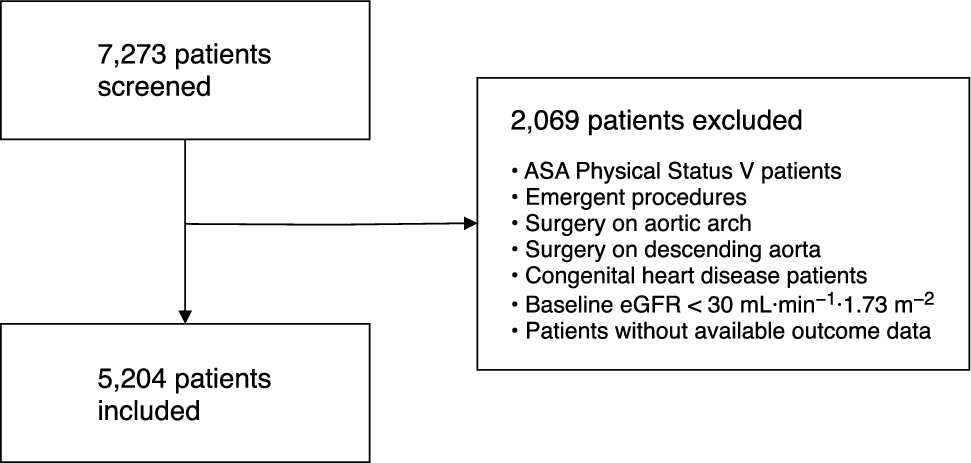
Selection of participantsBetween July 2023 and February 2024, we enrolled adult patients (aged ≥ 18 yr) who were scheduled for elective surgery requiring tracheal intubation under general anesthesia. We excluded patients with a history of cervical spine injury or pathology, absence of teeth, presence of loose teeth, unstable temporary teeth or partial dentures, periodontitis, oral abscess, craniofacial anomalies, history of difficult tracheal intubation, requirement for rapid sequence induction, or refusal to participate in the study.
RandomizationEach participant underwent two consecutive direct laryngoscopies using both the novel and conventional techniques. The patients were randomly assigned to one of the two groups according to the direct laryngoscopy technique used in the first attempt. In the novel technique group, direct laryngoscopy was initially performed using the novel technique, followed by the conventional technique. In the conventional technique group, the conventional technique was used first followed by the novel technique.
Randomization was performed using R software (version 4.2.0; R Foundation for Statistical Computing, Vienna, Austria) with a block size of two. The randomization results were placed in sealed opaque envelopes that were opened by a nurse who was not involved in the study, immediately before the induction of anesthesia.
Interventions and measurementsUpon arrival in the operating room, an anesthesiologist assessed each patient’s airway and dental conditions while they were in a seated position. The evaluation included the modified Mallampati classification,14 mandibular protrusion test,15 interincisor gap (mm), and thyromental distance (mm). The interincisor gap was measured with the patient’s mouth fully opened, and the thyromental distance was measured with the mouth closed and the head fully extended. The patient was then placed in a supine position with a 7 cm-high pillow. The maximum degree of neck extension was measured by calculating the difference in angle using a digital BevelBox (L.V. Level Co., Jiangsu, China) securely attached to the glabella in both neutral and fully extended neck positions.
Before induction of general anesthesia, the patients were monitored using pulse oximetry, electrocardiography, and noninvasive blood pressure measurements. After preoxygenation, anesthesia was induced with an intravenous bolus of 1.5–2 mg·kg−1 of propofol and continuous infusion of remifentanil through a target-controlled infusion (initial effect-site concentration of 3.0 ng·mL−1). Upon loss of consciousness, manual ventilation was initiated, and neuromuscular monitoring was started with a TwitchView device (Blink Device Company, Seattle, WA, USA) placed on the ulnar nerve at the wrist. The patients then received rocuronium 0.6–0.8 mg·kg−1iv to facilitate tracheal intubation. Anesthesia was maintained with sevoflurane, with a Bispectral Index™ (Medtronic, Minneapolis, MN, USA) of 40–60. When a train-of-four count of 0 was achieved, two consecutive laryngoscopies were performed in a randomized sequence. After the first laryngoscopy attempt, the patient’s head was promptly returned to a neutral position to minimize any potential impact on the second laryngoscopy. Tracheal intubation was performed only after the second laryngoscopy to minimize the risk of tracheal injury.
For the conventional technique, the laryngoscopy procedure was as follows: initially, the anesthesiologist used their right hand to maximally extend the patient’s head (T1). The laryngoscope was held in the left hand and aligned with the midline of the patient before insertion into the mouth. Subsequently, the laryngoscope was lifted upward and forward along the handle axis to ensure an optimal view of the glottis (T2). Finally, the right hand was released, and the optimal glottic view was maintained using only the necessary force of the left hand (T3C, Fig. 1A).
Fig. 1
Schematic illustration of head and neck positions during the tracheal intubation simulation. (A) The conventional laryngoscopy technique with the right hand withdrawn, maintaining optimal glottic view by left hand alone (T3C position; cf. body text). (B) The novel laryngoscopy technique using the left forearm or elbow to support the patient's forehead, maintaining head extension without the right hand (T3N position; cf. body text)
Angle α = the angle between the forehead line and the horizontal line; distance D = the shortest distance between the tip of the maxillary central incisors and the laryngoscopic blade; FH = force applied by the hand or forearm/elbow; FL = force applied by lifting the laryngoscope
While maintaining the T3C position, the research nurse who did not participate in the intervention recorded three measurements: dental contact with the maxillary incisors, blade-to-tooth distance, and angle of head extension. The blade-to-tooth distance was defined as the shortest vertical distance between the patient's upper incisor and the laryngoscope blade, which was measured using a ruler (Mitutoyo, Tokyo, Japan). The angle of head extension at T3 was calculated as the difference between the angle in the neutral neck position and that in the T3 position.
For the novel technique, the laryngoscopy procedure was performed in the same manner as in the conventional technique trial until T2. The patient’s head was then supported by the anesthesiologist’s left forearm or elbow to maintain an optimal glottic view, and the right hand was released (T3N, Fig. 1B). The measurements were performed in the same manner.
After completing intubation, the anesthesiologist who performed both laryngoscopies was asked to rate their satisfaction with each laryngoscopy using the percentage of glottic opening (POGO) score, which quantifies the proportion of glottic opening during laryngoscopy.16 The POGO score was converted to a 5-point scale: 1 (0–20%), 2 (21–40%), 3 (41–60%), 4 (61–80%), and 5 (81–100%).
Throughout the study, direct laryngoscopy was performed by two attending anesthesiologists (S. E. S. and J.-W. J.), both with no prior experience in the novel technique. The patient’s attending anesthesiologist selected a classic Macintosh blade (Dongguan Honfield Tape-Record Cassette Products Co., Ltd., Guangdong, China) with a size 3 or 4 blade on the basis of the patient’s sex. If the patient’s oxygen saturation dropped to below 90%, the procedure was immediately paused. The anesthesiologist then supplied 100% oxygen via mask ventilation until the peripheral oxygen saturation level was restored to > 98%. During the procedure, the attending anesthesiologist was instructed to prioritize minimizing dental contact while maintaining optimal intubation conditions to prevent TDI.
Outcome variables and statistical analysisThe primary outcome was the incidence of dental contact during each laryngoscopy. Secondary outcomes included blade-to-tooth distance (mm), angle of head extension (°), POGO score (1–5), and the proportion of laryngoscopy with high performer satisfaction (defined as a POGO score of 4 or 5).
Based on our previous study,11 we expected the incidence rate of dental contact to be 95% when using the conventional technique. We hypothesized that the novel technique would reduce the incidence rate to 75%, resulting in an improvement of approximately 20%. To calculate the sample size, we assumed a conservative discrepancy rate of 30% between the two techniques. We calculated a sample size of 75 participants using McNemar’s test, with a power of 0.9 and a two-sided alpha level of 0.05. Considering a 10% dropout rate, we planned to recruit 84 participants.
All statistical analyses were conducted using the R software (version 4.3.3; R Foundation for Statistical Computing, Vienna, Austria). We report categorical data as numbers (proportions); for comparison between the two techniques, we used McNemar’s test and present the results as relative risks and 95% confidence intervals (CIs).17 Continuous data are reported as mean (standard deviation [SD]) or median [interquartile range (IQR)] depending on the normality of the data distribution, as determined by the Shapiro–Wilk test; for comparisons, we used the paired t test or the Wilcoxon signed-rank test as appropriate. For non-normally distributed data, we calculated median differences and 95% CIs using the nonparametric percentile bootstrap method with 1,000 repetitions. We explored the potential for period and carryover effects for the primary outcome on the basis of a full model, incorporating treatment, period, and carryover effects, with a random intercept. Statistical significance was set at P < 0.05.
Comments (0)