Patients
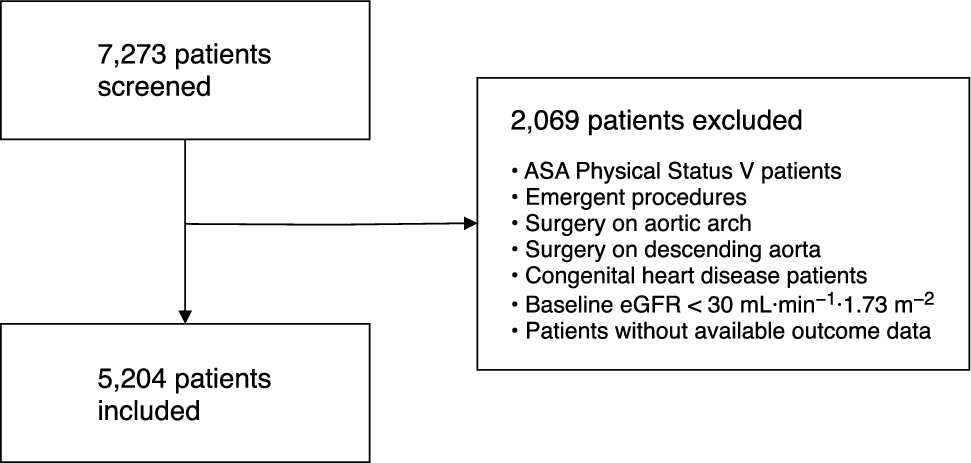
The present study is an observational post hoc study arising from the recent ALBICS trial. The ALBICS trial (ClinicalTrials.gov: NCT02560519) was a single-centre (Helsinki University Hospital, Helsinki, Finland), randomized, double-blind trial comparing 4% albumin (intervention group) and Ringer’s acetate (control group) as CPB priming solutions and intra- and postoperative volume replacement solutions in 1,386 adult patients undergoing on-pump cardiac surgery. The randomization was blinded to patients, study groups, study nurses, and personnel taking care of patients. Our previous publications have described the methodology in detail, including the inclusion and exclusion criteria, recruitment periods, follow-up, and data collection.18,20 The ALBICS trial was conducted according to the principles of the Declaration of Helsinki and was approved by the ethics committee of the Hospital District of Helsinki and Uusimaa, Helsinki, Finland (HUS/2917/2016 14.12.16/6.2.17/14.6.2017) and the Finnish Medicines Agency (Fimea; 136/2015, 25.11.2016 & 30.01.2017, EudraCT 2015-002556-27). We obtained written informed consent from the patients before surgery. This manuscript adheres to the applicable Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. A data analysis and statistical plan for the present post hoc study were written after the data for the main ALBICS study were accessed.
Trial intervention and patient care
The trial intervention comprised two phases conducted in a blinded fashion: 1) CPB priming (1,500 mL) and 2) intravenous volume replacement therapy (up to 3,200 mL) intraoperatively and during the first 24 postoperative hr. The Ringer’s group received Ringer’s acetate solution (RingerAcetat Baxter Viaflo®, Baxter Oy, Helsinki, Finland) in both phases. For CPB priming, the albumin group received a mixture of 20% albumin solution (Albuman® 200 mg·mL−1, Prothya Biosolutions, Amsterdam, Netherlands) and Ringer’s acetate solution, adjusted to a final albumin concentration of 4%. For intravenous volume replacement, the albumin group received 4% albumin solution (Albuman 40 mg·mL−1). Ringer’s acetate solution was administered in an unblinded fashion in both study groups if more than 3,200 mL of volume replacement was needed. Otherwise, patient care followed the standard clinical practice of the study site.
We performed CPB using a nonpulsatile pump and membrane oxygenator at mild hypothermia. The use of blood products, coagulation factor concentrates, and antifibrinolytics was based on clinical judgement. Tranexamic acid 1 g iv was typically given during anesthesia induction, and a second dose of 1 g iv at initiation of CPB. Clinical judgement guided the additional doses of tranexamic acid after CPB. The initial heparin dose was typically 300 IU·kg–1iv. We administered additional heparin boluses to maintain activated clotting time over 480 sec. After CPB, 1 mg of protamine per 100 IU of heparin was typically administered iv. The anesthesiologist retransfused the residual volume of the CPB circuit into the patient after CPB.
According to institutional practice, management of postoperative bleeding after cardiac surgery in the intensive care unit necessitated RBC transfusion for hematocrit < 30%, administration of platelets for platelet count < 100 × 109·L−1, and administration of fibrinogen concentrate for a plasma fibrinogen level < 1.5 g·L−1.
Blood samples and laboratory analyses
The study nurse collected arterial blood samples into tubes containing 3.2% sodium citrate (BD Vacutainer Citrate, Becton Dickinson Finland, Vantaa, Finland) before anesthesia induction (“preoperative”) and 30 min after protamine administration (“post-CPB”). Plasma was separated in the hospital laboratory at 2,500 × g for 15 min and stored at −80 °C until analyzed. We used preoperative plasma samples for the analysis of plasma fibrinogen levels and post-CPB plasma samples for the analyses of plasma fibrinogen levels, activated partial thromboplastin time (aPTT), and international normalized ratio (INR). Preoperative hematocrit, platelet count, aPTT, and INR were analyzed as part of the clinical routine at the preoperative anesthesia screening. The plasma fibrinogen level was analyzed with the Clauss method (normal range, 2.0–4.0 g·L−1), platelet count with impedance and flow cytometry particle count (normal range, 150–360 × 109·L−1), and aPTT with direct coagulation time measurement (normal range, 28–37 sec). INR was calculated from prothrombin time (PT) measured with the Owren method (normal range, 0.7–1.2) in the hospital laboratory. All coagulation parameters were measured with ACL TOP 500 (Instrumentation Laboratory, Werfen, Barcelona, Spain). Perioperative hematocrit was analyzed with an arterial blood gas analyzer (ABL90 Flex Plus, Radiometer, Turku, Finland).
Preoperatively, 1,336 plasma fibrinogen concentration, 1,382 platelet count, 1,268 aPTT, and 1,385 INR analyses were performed. The corresponding numbers for post-CPB analyses were 1,319 for plasma fibrinogen concentration, 1,317 for aPTT, and 1,319 for INR. Blood samples were collected consistently from all patients, but a small number of plasma samples were lost during storage.
Universal Definition of Perioperative Bleeding classification
To define severe perioperative bleeding, we used two dichotomous outcome measures based on the UDPB classification.17 First, we classified patients as UDPB-high (classes 3 and 4) vs UDPB-low (classes 0–2). Second, we divided patients according to resternotomy for bleeding, as defined in the UDPB classification. According to the classification, all patients with resternotomy were included in the category of UDPB-high. Blood products, coagulation factor concentrates, and resternotomy were accounted for from the cessation of CPB to the first 24 hr postoperatively. We accounted for chest tube drainage for the first 12 hr postoperatively.17
Statistical analysis
The study nurses or the study-specific IT application prospectively collected all data of this post hoc study of the ALBICS trial. The amount of missing data was low and random in nature. We did not impute missing data. We tested differences in continuous variables between two groups with Student’s t test and correlations between continuous variables with Pearson’s test. Fisher’s exact test was used to test for associations between two categorical variables. In multivariable logistic regression, we used variance inflation factor analysis to check for multicollinearity. We constructed two multivariable models for UDPB-high and resternotomy: 1) plasma fibrinogen level and standard hemostatic laboratory parameters (INR, aPTT, hematocrit, and platelet count), to study the predictive power of plasma fibrinogen levels in relation to other commonly used hemostatic laboratory parameters and 2) plasma fibrinogen levels and clinical risk factors of perioperative bleeding, detected previously in the multivariable analysis of the ALBICS cohort (age, body mass index, preoperative use of acetylsalicylic acid, ALBICS study group allocation, complex surgery, and urgent surgery),19 to study whether plasma fibrinogen levels carry an independent risk beyond preoperative risk factors for bleeding. We also constructed analogous multivariable models, including CPB time in addition to the variables mentioned above. We included all variables in the multivariable analysis irrespective of the significance levels in the univariable regression analyses.
We present results as mean and standard deviation (SD), frequency and proportion, or odds ratio (OR) and 95% confidence interval (CI). Odds ratios for continuous variables are expressed as per SD. For comparability between preoperative and postoperative laboratory measurements, preoperative SDs were also used for postoperative ORs. We considered a two-sided P value of < 0.05 statistically significant. We conducted statistical analyses with IBM SPSS Statistics version 28 software (IBM Corp., Armonk, NY, USA).



Comments (0)